Antibiotics in Dentistry: Complete Guide for Dental Infections, Dosage, Side Effects & Resistance (2026)
TL;DR
- Most dental infections do not require antibiotics yet dentistry contributes nearly 10% of total antibiotic prescriptions in India, with 20–50% considered unnecessary
- Antibiotics do not treat dental pain. They only help control bacterial spread temporarily
- First-line: Amoxicillin (± clavulanic acid). Alternatives: Azithromycin, Clindamycin, Cephalosporins.Duration: Typically 3–5 days (review-based)
- Overuse leads to: antibiotic resistance, treatment failure and higher healthcare costs. The real treatment remains drainage, root canal treatment (RCT), and extraction.
Do you really need antibiotics for tooth pain?
This is the biggest myth in dentistry. Most patients and even some practitioners believe: “Tooth pain = antibiotics”
This assumption feels logical. Pain usually signals infection. Antibiotics treat infections. So the connection seems obvious. But clinically, this is where things go wrong.
The Reality
Antibiotics do not remove the source of dental infection; they only temporarily reduce bacterial activity.
Let’s break this down in a real scenario you see every day:
- A decayed tooth leads to pulp infection
- Pressure builds inside a closed space
- Pain develops
If you prescribe antibiotics:
- bacterial load may reduce temporarily
- inflammation may decrease slightly
But: The infected pulp remains untreated
Until you perform:
- root canal treatment
- or extraction
The infection persists
That is why many patients report:
- pain relief during medication
- recurrence after stopping antibiotics
This is not treatment failure, it is incomplete treatment.
The Bigger Problem in India
This misunderstanding is not isolated, it scales into a national issue.
Recent data shows:
- Dentistry contributes ~10% of total antibiotic prescriptions in India
- Around 20–30% (up to 50%) are unnecessary
- Self-medication rates for dental problems range from 5–35%
At the same time:
- India carries one of the highest antimicrobial resistance (AMR) burdens globally
- Resistance is rising in common oral pathogens like:
- Streptococcus
- Staphylococcus
This creates a compounding problem: Overprescription today → ineffective antibiotics tomorrow
As the Indian Council of Medical Research highlights in recent surveillance reports, resistance in community-acquired infections including dental sources is steadily increasing, especially for commonly used drug classes.
What Are Dental Antibiotics?
Definition-
Dental antibiotics are medications used to control bacterial infections not to eliminate the source of infection or relieve pain directly.
What They Are Used For
In clinical practice, antibiotics are indicated to:
- control spreading infections
- prevent systemic involvement
- support treatment in severe or high-risk cases
They are particularly relevant when:
- infection extends beyond the tooth
- systemic symptoms are present
What They Are NOT Used For
This is where clarity is critical.
Antibiotics are not indicated for:
- simple toothache
- reversible or irreversible pulpitis
- localized abscess (if drainage is possible)
- routine dental procedures
Using antibiotics in these cases does not improve outcomes; it delays proper care.
Key Clinical Principle
Antibiotics are adjuncts, not primary treatment. This principle is consistently emphasized in global and Indian guidelines.
As noted in stewardship reviews:
“Definitive dental treatment such as drainage or root canal therapy should be the primary approach, with antibiotics reserved for systemic involvement or spreading infections.”
When Are Antibiotics Needed in Dentistry?
Understanding indications is where clinical judgment matters most.
When You SHOULD Use Antibiotics
Antibiotics are justified when there is evidence of systemic spread or risk:
- facial swelling
- cellulitis
- fever and malaise
- spreading infection
- immunocompromised patients
- post-surgical infections
In these cases: Infection is no longer localized it becomes a systemic concern
When Antibiotics Are NOT Needed
In most routine dental conditions:
- simple toothache
- localized abscess (manageable with drainage)
- pulpitis
- routine extractions
Local treatment alone is sufficient
Clinical Rule
Most dental infections require mechanical intervention not pharmacological management
This is the difference between:
- treating symptoms
- and resolving disease
Antibiotics Used in Dentistry, Complete Clinical Breakdown
Dental antibiotics are selected based on infection severity, bacterial profile, patient history, and resistance patterns. In India, while multiple classes are used, clinical guidelines consistently prioritize narrow-spectrum agents as first-line therapy, with broader drugs reserved for specific or resistant cases.
What you need to understand here is simple: Not all antibiotics are equal and not all infections require the same level of coverage
Let’s break this down in a way that reflects real clinical decision-making, not just textbook listing.
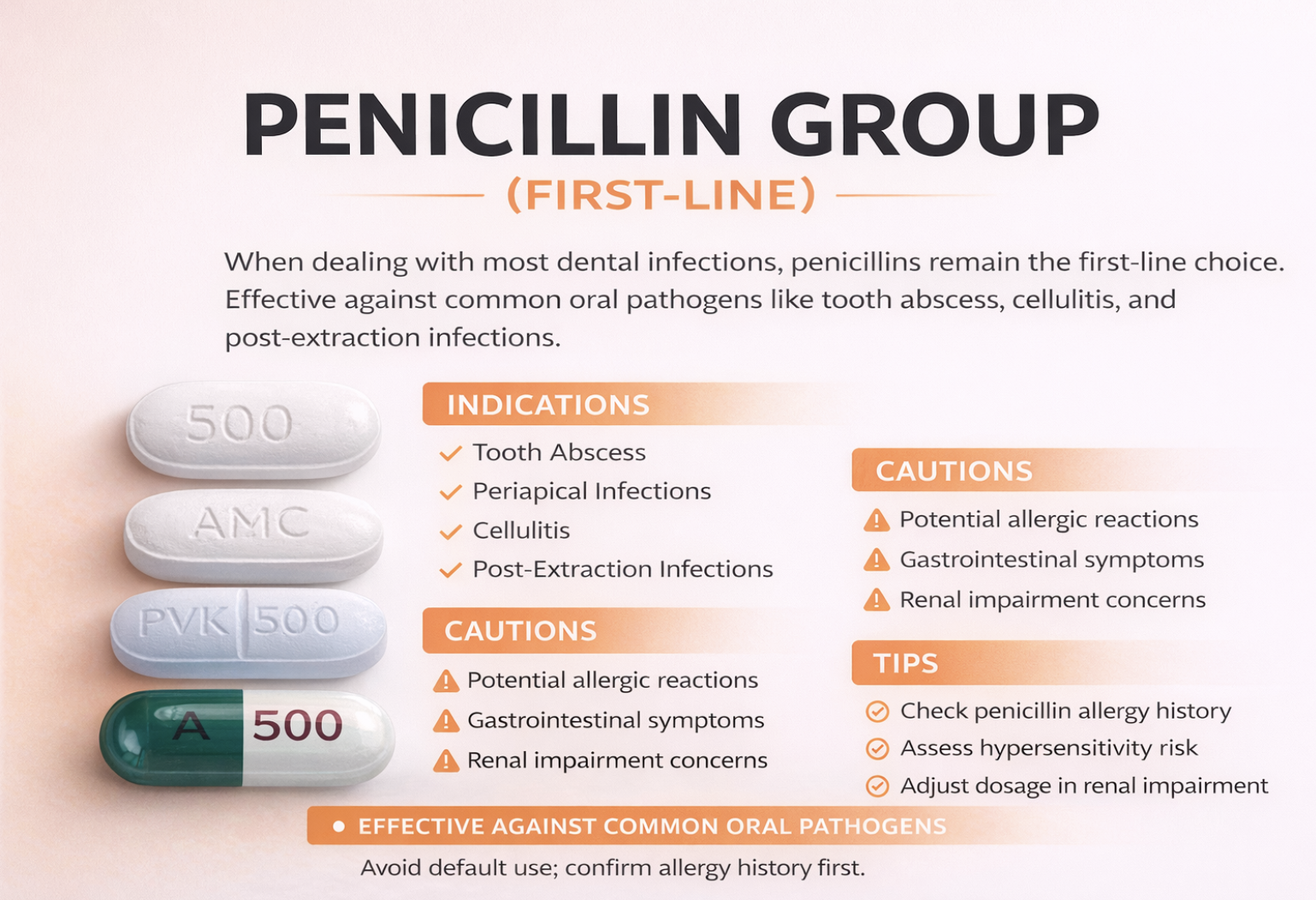
1. Penicillin Group (First-Line)
When you are dealing with most dental infections, penicillins remain the first-line choice. This is because they are effective against the common oral pathogens and have a well-established safety profile.
This group includes widely used drugs such as amoxicillin, amoxicillin with clavulanic acid, penicillin VK, ampicillin, and ampicillin-sulbactam. In everyday practice, you’ll see amoxicillin being prescribed most frequently, with clavulanic acid added when broader coverage is needed.
Clinically, these are used in conditions like:
- tooth abscess
- periapical infections
- cellulitis
- post-extraction infections
However, while effective, they are not risk-free. Patients may experience allergic reactions ranging from mild rash to severe anaphylaxis, along with gastrointestinal symptoms like diarrhea and nausea.
This is why, before prescribing, you must:
- carefully check penicillin allergy history
- assess hypersensitivity risk
- adjust dosage in patients with renal impairment
In practice, penicillins work best when used early, appropriately, and only when indicated not as a default prescription.
2. Cephalosporins
Cephalosporins are often considered when penicillins cannot be used or when you need slightly broader coverage in mild to moderate infections.
Common examples include cephalexin, cefadroxil, cefixime, cefuroxime, and cephradine. These are particularly useful in patients who do not tolerate penicillins well but do not have severe allergies.
You’ll typically use them for:
- mild to moderate odontogenic infections
- alternative therapy in selected patients
That said, one critical factor you must consider is cross-reactivity with penicillin allergy, especially in patients with a history of severe reactions.
Side effects are generally milder but still include:
- gastrointestinal discomfort
- mild allergic responses
The key here is judgment. Cephalosporins are not first-line replacements; they are context-based alternatives.
3. Macrolides (For Penicillin Allergy)
When a patient has a confirmed penicillin allergy, macrolides become a practical option. Drugs like azithromycin, clarithromycin, and erythromycin are commonly used in such cases.
These are typically prescribed for:
- mild dental infections
- patients unable to take beta-lactam antibiotics
From a clinical standpoint, azithromycin is often preferred due to its shorter course and better patient compliance.
However, macrolides come with important considerations. Patients may experience:
- nausea
- abdominal discomfort
More importantly: There is a known risk of QT interval prolongation, which can affect cardiac rhythm.
So in patients with:
- cardiac conditions
- existing arrhythmias
- interacting medications
You need to proceed with caution.
4. Nitroimidazoles (Anaerobic Coverage)
Dental infections are often anaerobic in nature, which is where nitroimidazoles like metronidazole, tinidazole, and ornidazole become highly relevant.
These are especially useful in:
- periodontal infections
- deep anaerobic infections
- cases where standard antibiotics need support
In many cases, you will not use them alone but in combination with penicillin to achieve broader bacterial coverage.
Patients commonly report:
- metallic taste
- nausea
- mild headache
But the most important precaution remains: Strict avoidance of alcohol due to adverse reactions
In real practice, metronidazole is often the “supporting drug”, not the primary one.

5. Lincosamides
When infections become severe or when both penicillin and alternatives are not suitable clindamycin is often considered.
It is particularly useful in:
- severe odontogenic infections
- osteomyelitis
- penicillin-allergic patients with higher risk infections
Clindamycin has strong bone penetration, which makes it clinically valuable in complex cases. However, this benefit comes with a serious risk:
Clostridioides difficile (C. diff) infection, which can lead to severe gastrointestinal complications
Patients may also experience:
- diarrhea
- abdominal discomfort
Because of this, clindamycin should never be used casually; it is a reserved drug for specific scenarios.
6. Fluoroquinolones
Fluoroquinolones such as ciprofloxacin, ofloxacin, and levofloxacin are not standard dental antibiotics, but they may be used in resistant or complicated infections.
These are typically considered when:
- standard therapies fail
- infection is polymicrobial or resistant
However, their safety profile demands caution. Known side effects include:
- dizziness
- central nervous system effects
And more seriously: Risk of tendon rupture, particularly in older patients
Because of these risks:
- they should be avoided in children and pregnancy
- they are not first-line choices
Think of fluoroquinolones as last-resort options, not routine prescriptions.
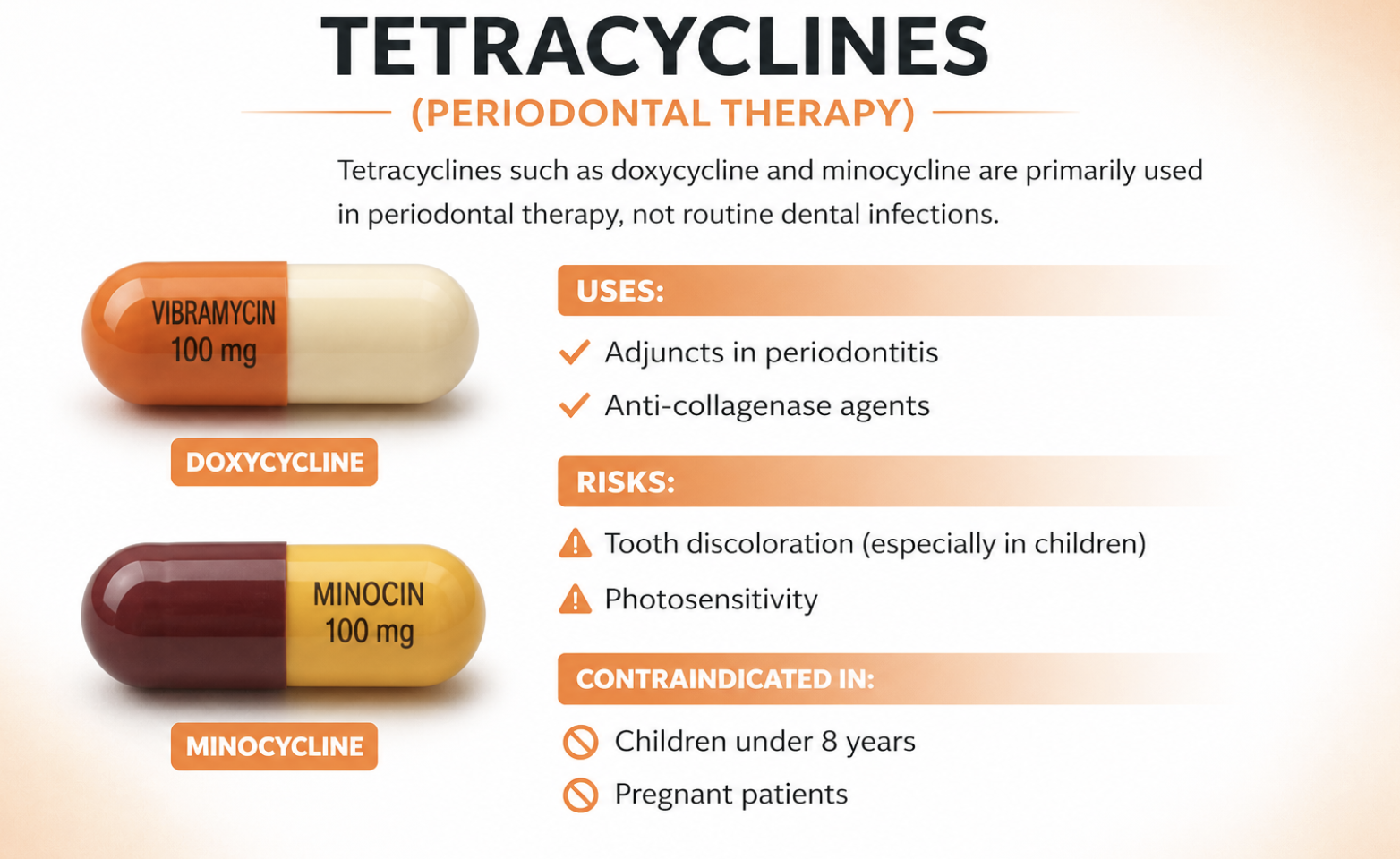
7. Tetracyclines
Tetracyclines such as doxycycline and minocycline are primarily used in periodontal therapy, not routine dental infections.
They are valuable as:
- adjuncts in periodontitis
- anti-collagenase agents
However, they come with well-known risks:
- tooth discoloration (especially in children)
- photosensitivity
Which means:
They must be avoided in:
- children under 8 years
- pregnant patients
8. Sulfonamides
Sulfonamides like co-trimoxazole are rarely used in dentistry today but may still appear in specific resistant cases.
Their use is limited due to:
- risk of hypersensitivity
- availability of better alternatives
Patients may develop:
- skin rashes
- allergic reactions
These are not routine drugs, they are situational choices.

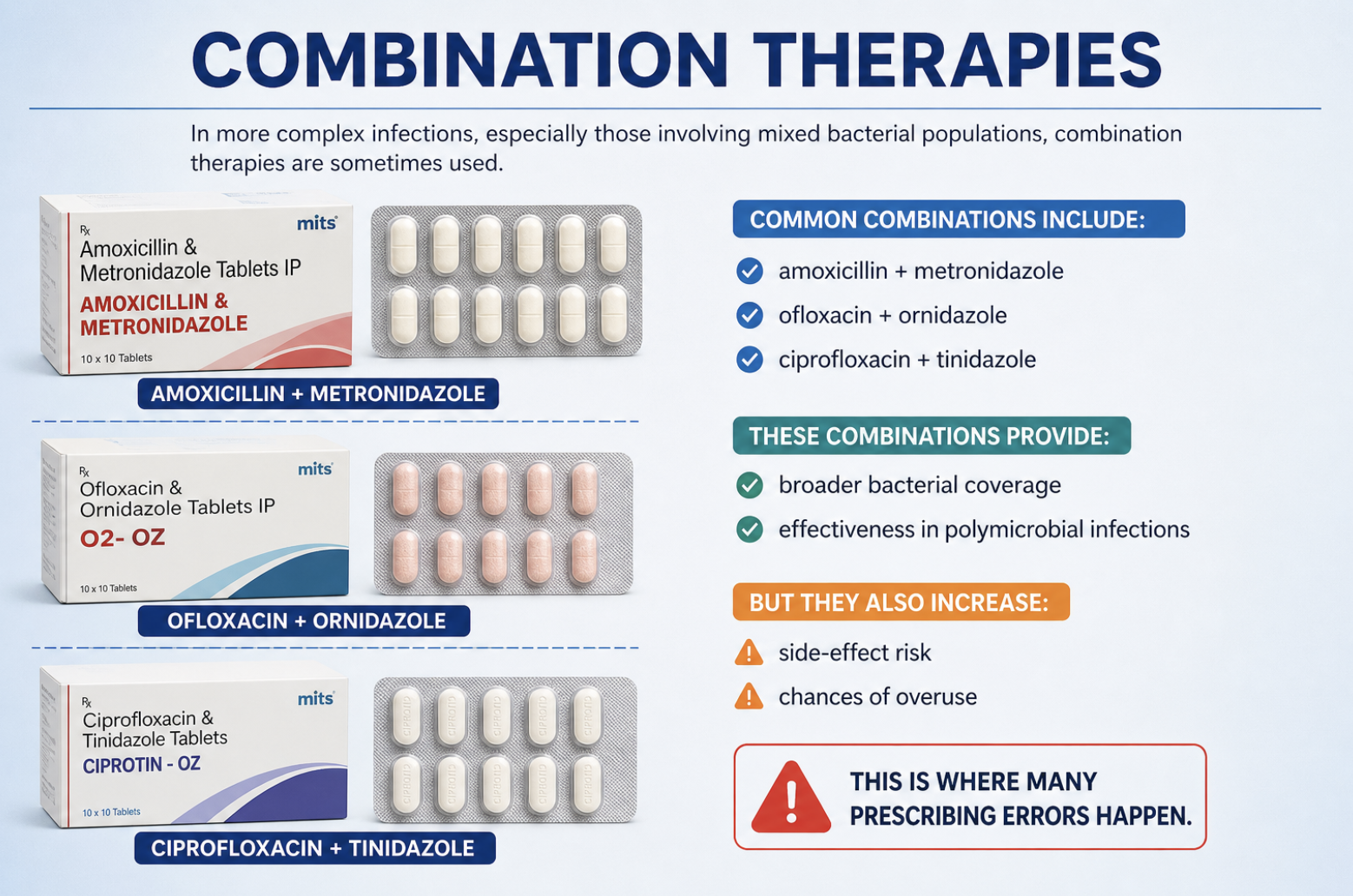
9. Combination Therapies
In more complex infections, especially those involving mixed bacterial populations, combination therapies are sometimes used.
Common combinations include:
- amoxicillin + metronidazole
- ofloxacin + ornidazole
- ciprofloxacin + tinidazole
These combinations provide:
- broader bacterial coverage
- effectiveness in polymicrobial infections
But they also increase:
- side-effect risk
- chances of overuse
This is where many prescribing errors happen.
Final Clinical Insight
When you step back, a clear pattern emerges:
- Most dental infections respond to simple, narrow-spectrum antibiotics
- Overuse of broad-spectrum and combinations is often unnecessary
And this aligns directly with recent India data: Broad-spectrum antibiotics are used in 20–30% of cases where they are not required.
The Real Takeaway
You don’t need more antibiotics.
You need better antibiotic decisions.
Right drug
Right indication
Right duration
Because in dentistry:
The goal is not to suppress infection
It is to eliminate its source with antibiotics only supporting that process
Antibiotic Classes in Dentistry
| Class | Common Drugs | Use Case | Key Risks |
| Penicillins | Amoxicillin, Amox-Clav | First-line infections | Allergy |
| Cephalosporins | Cefixime, Cephalexin | Mild–moderate infections | Cross-reactivity |
| Macrolides | Azithromycin | Penicillin allergy | QT prolongation |
| Nitroimidazoles | Metronidazole | Anaerobic infections | Alcohol interaction |
| Lincosamides | Clindamycin | Severe infections | C. difficile |
| Fluoroquinolones | Ciprofloxacin | Resistant cases | Tendon rupture |
| Tetracyclines | Doxycycline | Periodontal therapy | Tooth discoloration |
You’ll notice a pattern: Most broad-spectrum drugs are not first-line. This is where stewardship becomes critical.
Antibiotic Resistance in India: The Real Threat
Antibiotic resistance is no longer a future risk; it is already affecting treatment outcomes today.
What the Data Shows
Recent findings highlight:
- India is among the largest consumers of antibiotics globally
- Over 40–60% resistance rates reported in common pathogens for certain drug classes
- Dental prescribing contributes significantly to community-level exposure
Global projections indicate: Up to 10 million deaths annually by 2050 due to AMR with India bearing a substantial share.
What This Means in Practice
For you as a clinician:
- infections become harder to treat
- standard drugs lose effectiveness
- stronger, more toxic drugs may be required
For patients:
- longer recovery times
- increased complications
- higher costs
Antibiotic misuse today = treatment failure tomorrow
Best Practices for Dentists
To manage infections effectively while reducing resistance:
Always Prioritize
- drainage
- root canal treatment
- extraction
These remove the source of infection.
Use Antibiotics Only When
- systemic involvement exists
- infection is spreading
- patient is high-risk
Prescription Principles
- short duration: 3–5 days
- reassess before extending
- prefer narrow-spectrum drugs
Studies show: Stewardship programs can reduce unnecessary use by 20–30%
Common Mistakes in Dental Antibiotic Use
Even experienced practitioners can fall into patterns that increase misuse.
Frequent Errors
- prescribing antibiotics for pain
- overprescribing after extractions
- ignoring allergy history
- using broad-spectrum unnecessarily
- not completing definitive treatment
Why These Mistakes Matter
Each of these leads to:
- temporary relief
- delayed treatment
- increased resistance
Antibiotics without treatment = temporary suppression, not cure.
India-Specific Challenges
The issue is not just clinical, it is systemic.
1. OTC Misuse
Patients often:
- self-medicate
- stop courses early
- reuse old prescriptions
This accelerates resistance.
2. Access Gaps
- delayed dental visits
- reliance on pharmacies
- lack of specialist access
3. Awareness vs Practice Gap
While many dentists understand AMR:
Only 30–40% consistently change prescribing behavior.
4. Lack of Standardization
- inconsistent guidelines
- variation in prescribing patterns
- limited audit systems
The Future: Antibiotic Stewardship in Dentistry
The next phase of dentistry is not just treatment, it is responsible prescribing.
What Needs to Change
- guideline-based prescribing
- narrow-spectrum preference
- culture-based therapy in complex cases
The Direction
Modern systems are moving toward:
- evidence-based dentistry
- digital decision support
- integrated stewardship frameworks
Research shows: Structured stewardship can reduce misuse by 20–30% in dental settings.
Final Insight
Antibiotics are powerful but they are limited. They do not fix dental infections, dentists do.
And the distinction matters:
Treatment removes infection.
Antibiotics only support it.
Continue Learning & Explore Expert Dental Insights
If you’ve made it this far, you already understand something most people don’t: Antibiotics are not the solution to dental infections, correct diagnosis and treatment are.
But the real challenge is this: How do you stay updated with evidence-based dentistry without relying on outdated practices or guesswork?
For dentists, students, and healthcare professionals who want clinically accurate, research-backed insights on dental imaging, diagnosis, and treatment: Explore more expert-driven content on the Nidaan Dental Blog.
Because in modern dentistry: Better decisions start with better data and better understanding not more medication.
FAQs
1. Do antibiotics cure dental infections?
No, antibiotics do not cure dental infections. They only help control bacterial spread temporarily. The actual source of infection such as infected pulp or abscess must be treated through procedures like root canal treatment, drainage, or extraction. Without this, the infection is likely to return.
2. When should antibiotics be prescribed for dental infections?
Antibiotics are recommended only when there is systemic involvement or spreading infection, such as:
- facial swelling
- fever or malaise
- cellulitis
- compromised immunity
For localized infections, mechanical treatment alone is usually sufficient.
3. Which is the most commonly used antibiotic in dentistry?
The most commonly prescribed antibiotic is amoxicillin, often considered first-line for dental infections. In some cases, it may be combined with clavulanic acid to extend its effectiveness against resistant bacteria.
4. Are antibiotics necessary for tooth pain?
No, antibiotics are not required for tooth pain alone. Pain is usually caused by inflammation or infection within the tooth, which must be treated with dental procedures not medication. Antibiotics do not relieve pain directly.
5. What happens if dental antibiotics are overused?
Overuse of antibiotics can lead to:
- antibiotic resistance
- reduced effectiveness of common drugs
- recurrent or harder-to-treat infections
- increased healthcare costs
In India, studies show that 20–50% of dental antibiotic prescriptions may be unnecessary, contributing to this growing problem
6. How long should antibiotics be taken for dental infections?
Typically, antibiotics are prescribed for 3–5 days, depending on the severity of infection. Dentists often reassess the condition before extending the course. Prolonged or unnecessary use increases the risk of resistance.
7. Can I stop antibiotics once I feel better?
No, you should not stop antibiotics early unless advised by your dentist. Incomplete courses can:
- allow bacteria to survive
- increase resistance
- lead to recurrence of infection
Always follow the prescribed duration.
8. What are the common side effects of dental antibiotics?
Common side effects include:
- nausea and vomiting
- diarrhea
- abdominal discomfort
- allergic reactions (in some cases)
Certain antibiotics may have specific risks, such as:
- QT prolongation (macrolides)
- C. difficile infection (clindamycin)
- tendon injury (fluoroquinolones)
9. Can antibiotics replace root canal treatment?
No, antibiotics cannot replace root canal treatment. They do not remove infected tissue inside the tooth. Without proper treatment, the infection will persist and often worsen over time.
10. Why is antibiotic resistance a major concern in dentistry?
Antibiotic resistance makes infections harder to treat and reduces the effectiveness of commonly used drugs. In India:
- dental prescriptions contribute significantly to overall antibiotic use
- resistance is rising in common oral bacteria
This means future infections may require stronger, more toxic, and more expensive medications.
11. What is the safest way to use antibiotics in dentistry?
The safest approach includes:
- prescribing only when clinically indicated
- choosing narrow-spectrum antibiotics whenever possible
- limiting duration (3–5 days)
- combining with definitive treatment (RCT, drainage, extraction)
This approach aligns with modern antibiotic stewardship principles.
12. Can I take antibiotics without consulting a dentist?
No, self-medication is strongly discouraged. In India, 5–35% of patients self-medicate for dental issues, which increases the risk of incorrect drug use, incomplete treatment, and antibiotic resistance
Always consult a qualified dentist before taking antibiotics.