TL;DR
- OPG provides a broad overview of the jaws, teeth, TMJs, and surrounding structures.
- CBCT provides detailed 3D visualization of bone, nerves, roots, sinuses, and pathology.
- OPG is generally lower in cost and radiation exposure.
- CBCT is preferred for implant planning, impacted teeth localization, complex endodontics, pathology evaluation, and surgical planning.
- Professional guidelines continue to recommend CBCT only when additional information will influence diagnosis or treatment.
- Around 80–85% of general dentists still use OPG as their primary screening modality, even when CBCT is available.
- Approximately 25–30% of planned CBCT scans are modified or cancelled after initial OPG review, demonstrating the continuing value of panoramic imaging.
Most patients who visit a dental clinic do not need a CBCT scan first. In fact, OPG (Orthopantomogram) remains the preferred first-line imaging modality for routine dental examinations, orthodontic assessment, wisdom tooth evaluation, and general diagnosis. CBCT (Cone Beam Computed Tomography) becomes valuable when treatment decisions depend on accurate three-dimensional anatomical information.
How Do You Know Whether You Need a CBCT Scan or an OPG Scan?
Direct Answer
CBCT is the preferred scan when treatment planning depends on precise three-dimensional anatomical information. OPG remains the preferred first-line imaging modality for routine screening, orthodontic assessment, wisdom tooth evaluation, and general dental diagnosis because it provides a broad overview quickly, efficiently, and with lower radiation exposure.
A practical clinical rule is simple: OPG for overview. CBCT for precision. The goal is not to order the most advanced scan available. The goal is to order the scan that answers the clinical question accurately while avoiding unnecessary radiation, cost, and complexity.
Why Does the Choice Between CBCT and OPG Matter More Than Ever?
Modern dentistry has entered an era where advanced imaging is widely available. Many practices now have access to both panoramic imaging and CBCT technology. This has created an important shift in clinical decision-making.
The question is no longer: “Can we perform a CBCT scan?”
The real question is: “Should we perform a CBCT scan?”
As access to three-dimensional imaging increases, clinicians carry greater responsibility to justify every radiographic examination. Evidence-based dentistry consistently supports the principle that imaging should only be prescribed when it contributes meaningful information to diagnosis or treatment planning.
This explains why panoramic imaging continues to play a critical role in daily dental practice despite the rapid growth of CBCT technology.
Recent industry data shows that approximately 80–85% of general dentists continue to use OPG as their primary screening modality, even when CBCT systems are available. In addition, nearly 25–30% of initially proposed CBCT examinations are altered or cancelled after reviewing an OPG first, highlighting how often panoramic imaging alone can answer the clinical question.
The lesson is simple: The most advanced technology is not automatically the best choice. The best imaging modality is the one that provides the information necessary for patient care.
What Is an OPG Scan?
An OPG (Orthopantomogram) is a two-dimensional panoramic dental X-ray that captures the entire oral and maxillofacial region in a single image. Unlike intraoral radiographs that focus on a small area, panoramic imaging provides a comprehensive overview of both jaws and surrounding anatomical structures.
A standard OPG typically visualizes:
- Maxilla and mandible
- Full dentition
- Alveolar bone
- Temporomandibular joints (TMJ)
- Condyles
- Maxillary sinuses
- Impacted teeth
- General skeletal structures
Because of this wide field of view, OPG has become the diagnostic foundation of routine dentistry.
Why OPG Remains the First-Line Imaging Modality
The continued relevance of panoramic imaging is driven by practicality rather than tradition. An OPG provides a significant amount of diagnostic information while remaining:
| Advantage | Clinical Benefit |
| Broad anatomical coverage | Entire jaws and dentition visible |
| Fast acquisition | Completed within seconds |
| Lower radiation exposure | Less exposure than CBCT |
| Cost-effective | Accessible for most patients |
| Excellent screening tool | Multiple structures assessed simultaneously |
For routine dental assessments, clinicians often need a broad overview rather than highly detailed anatomical measurements. OPG provides exactly that.
This makes it particularly valuable for:
- New patient examinations
- Treatment planning discussions
- Referral assessments
- Preventive screening
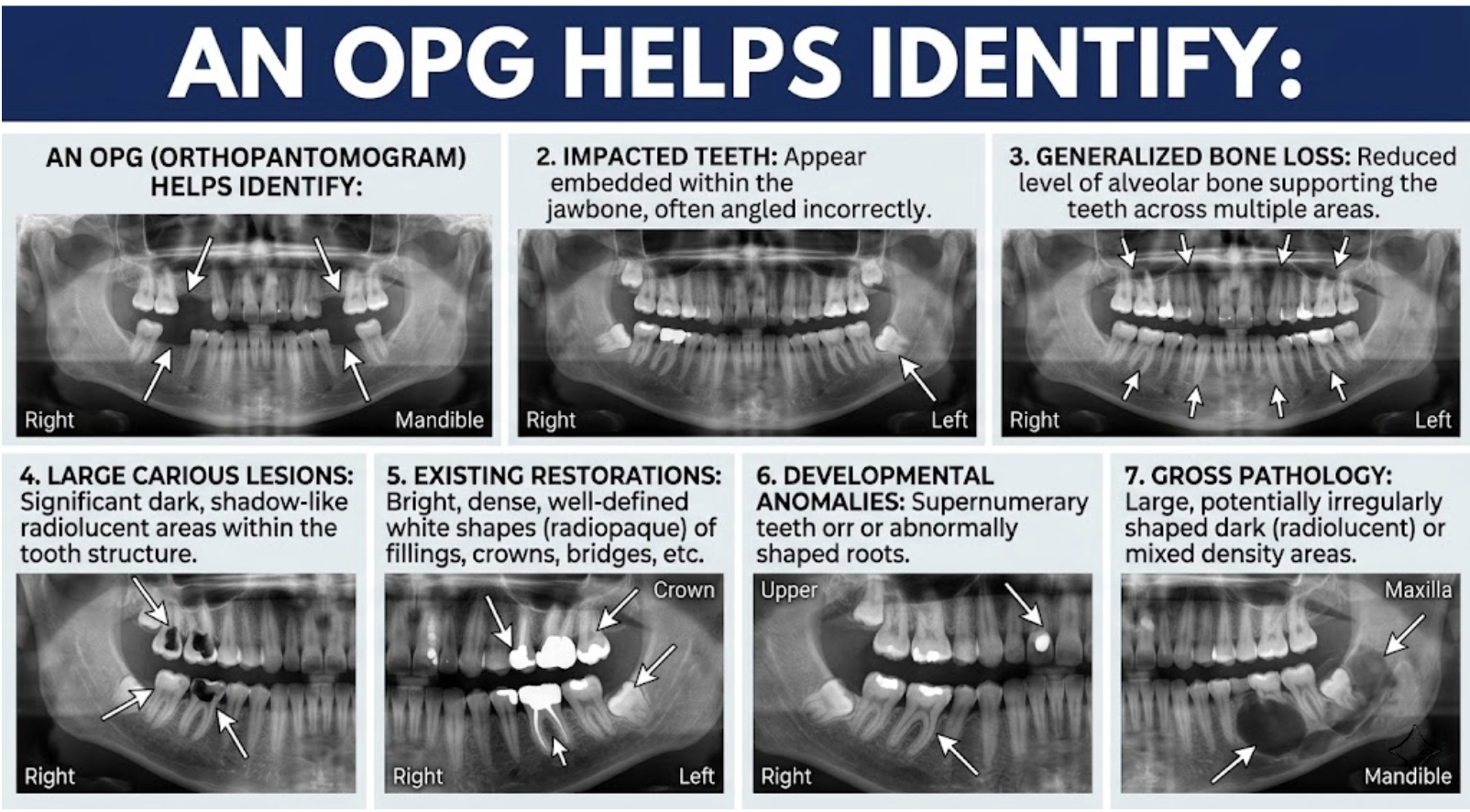
Common Clinical Applications of OPG
General Dental Assessment
When a patient attends a dental clinic for an initial evaluation, clinicians often need to understand the overall condition of the oral cavity before making treatment recommendations.
An OPG helps identify:
- Missing teeth
- Impacted teeth
- Generalized bone loss
- Large carious lesions
- Existing restorations
- Developmental anomalies
- Gross pathology
This broad perspective allows clinicians to prioritize treatment and identify areas requiring further investigation.
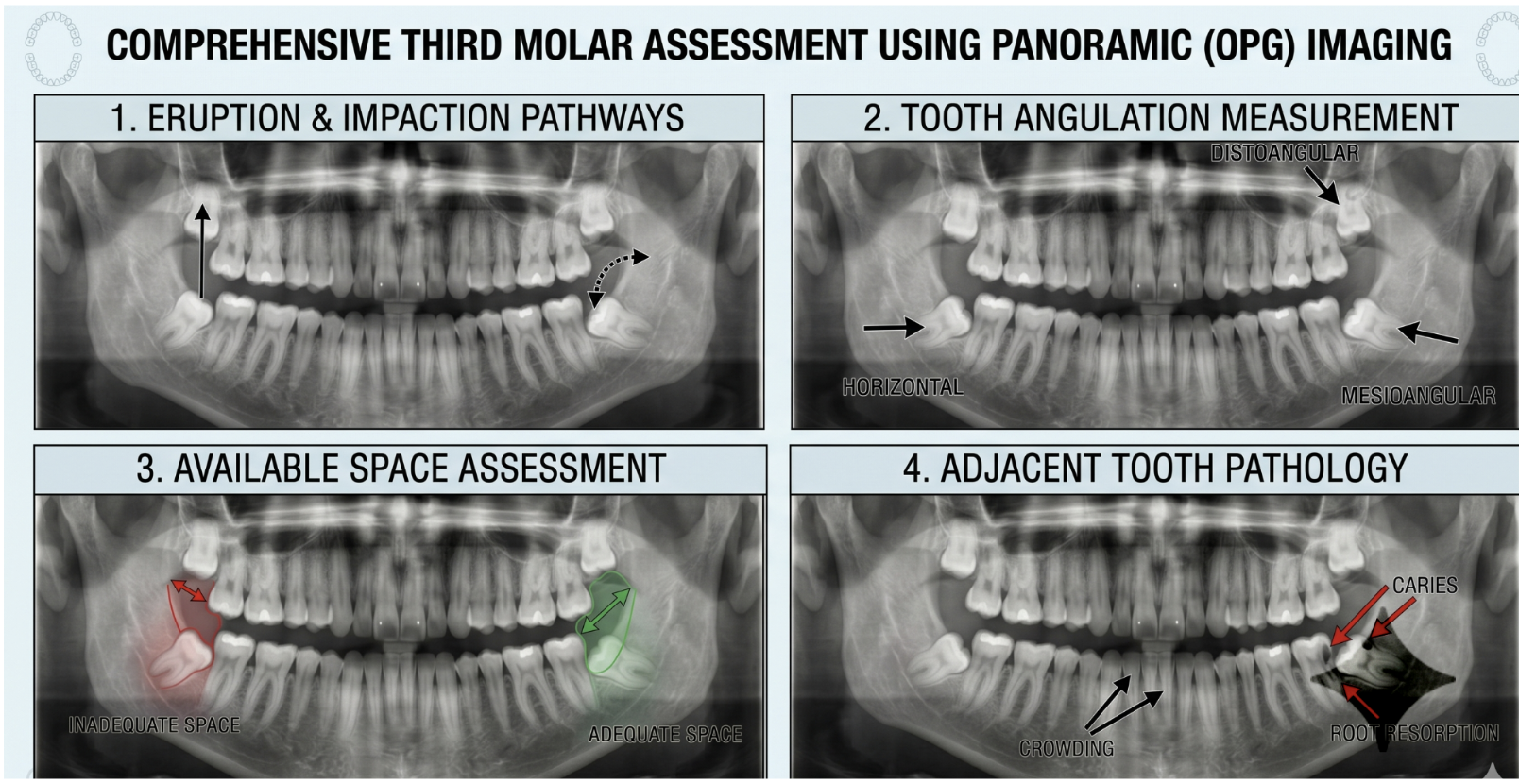
Wisdom Tooth Evaluation
Third molar assessment remains one of the most common indications for panoramic imaging. An OPG allows dentists to evaluate:
- Eruption patterns
- Tooth angulation
- Available space
- Relationship to adjacent teeth
In many straightforward cases, this information is sufficient for clinical decision-making.
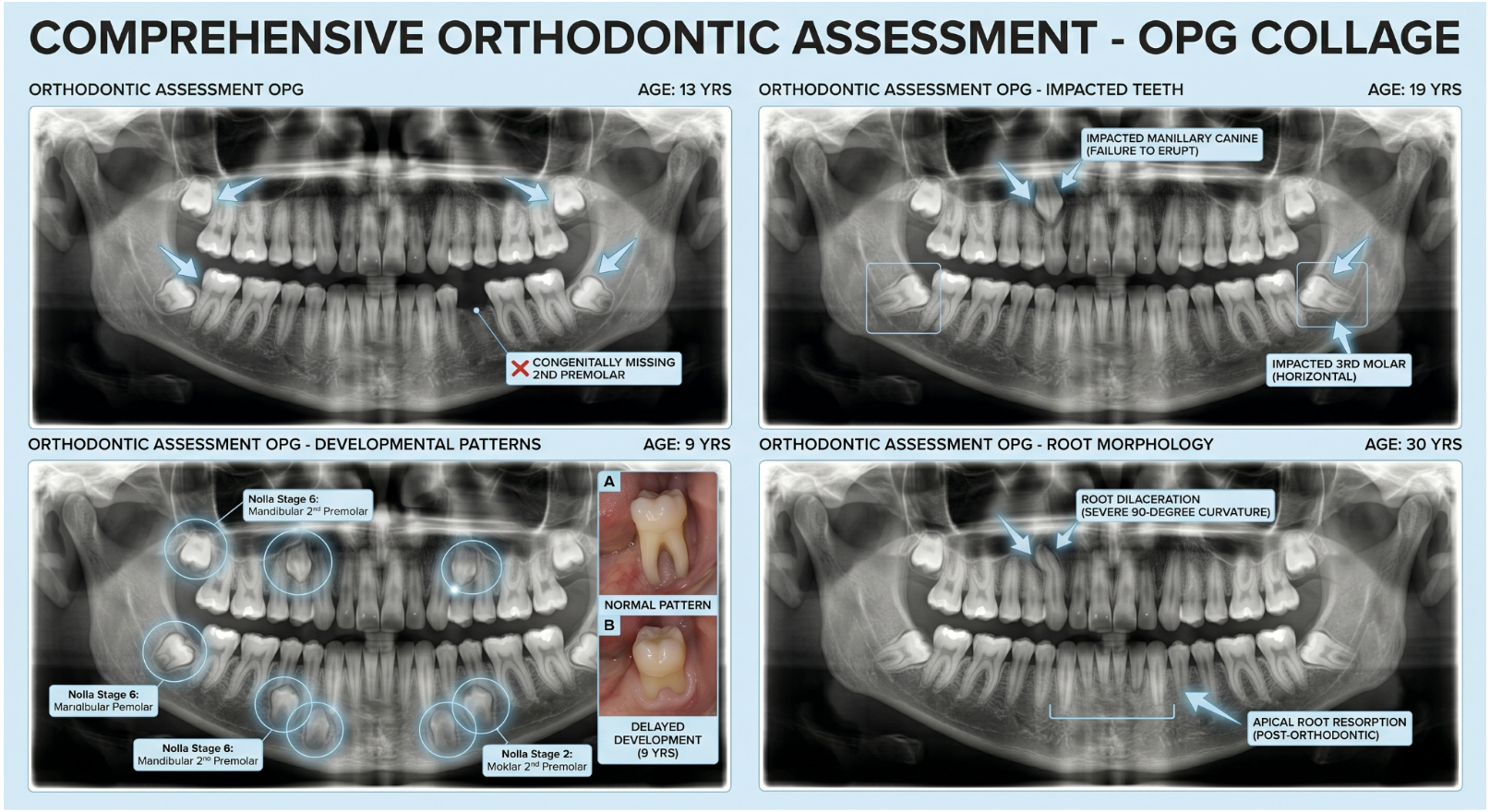
Orthodontic Assessment
Panoramic radiography remains an important component of orthodontic records. Combined with cephalometric imaging, OPG supports evaluation of:
- Tooth eruption
- Root morphology
- Impacted teeth
- Missing teeth
- Developmental patterns
For most routine orthodontic cases, this information is adequate for treatment planning.
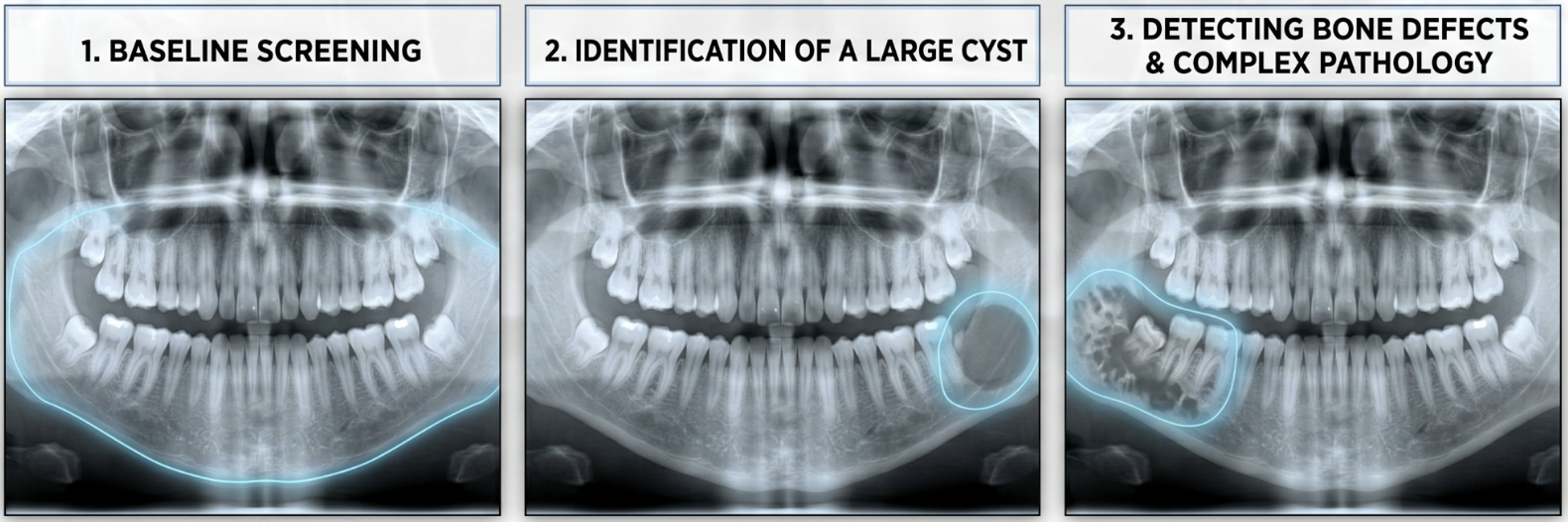
Pathology Screening
Although CBCT often becomes necessary for detailed pathology assessment, OPG frequently serves as the first imaging study that identifies abnormalities.
It is useful for detecting:
- Large cysts
- Gross lesions
- Bone defects
- Impacted teeth
- Developmental abnormalities
This screening capability explains why panoramic imaging continues to form the backbone of many referral workflows.
What Is a CBCT Scan?
CBCT (Cone Beam Computed Tomography) is a three-dimensional imaging modality that reconstructs oral and maxillofacial anatomy into a volumetric dataset. Instead of compressing anatomical structures into a flat image, CBCT allows clinicians to evaluate anatomy from multiple planes and angles.
This eliminates one of the biggest limitations of conventional radiography: Anatomical superimposition. Structures that overlap on a panoramic image can be isolated and viewed individually within a CBCT dataset.
This capability fundamentally changes how clinicians assess risk, plan surgery, and evaluate anatomy.
What Information Can CBCT Reveal?
A CBCT scan provides detailed visualization of structures that are difficult or impossible to evaluate accurately on panoramic radiographs alone.
These include:
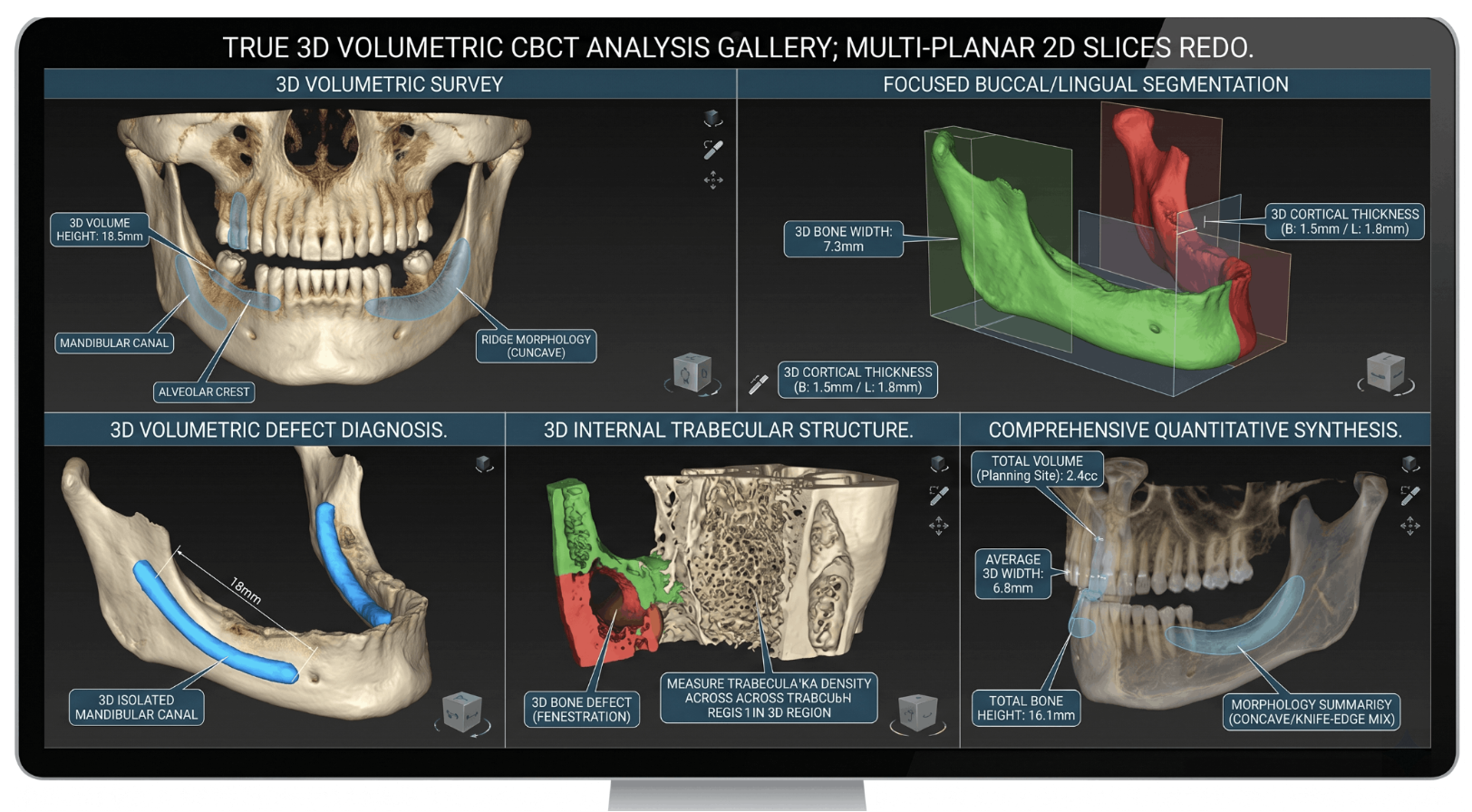
Bone Assessment
Clinicians can evaluate:
- Bone height
- Bone width
- Cortical thickness
- Ridge morphology
- Bone defects
This information is essential when precise measurements influence treatment outcomes.
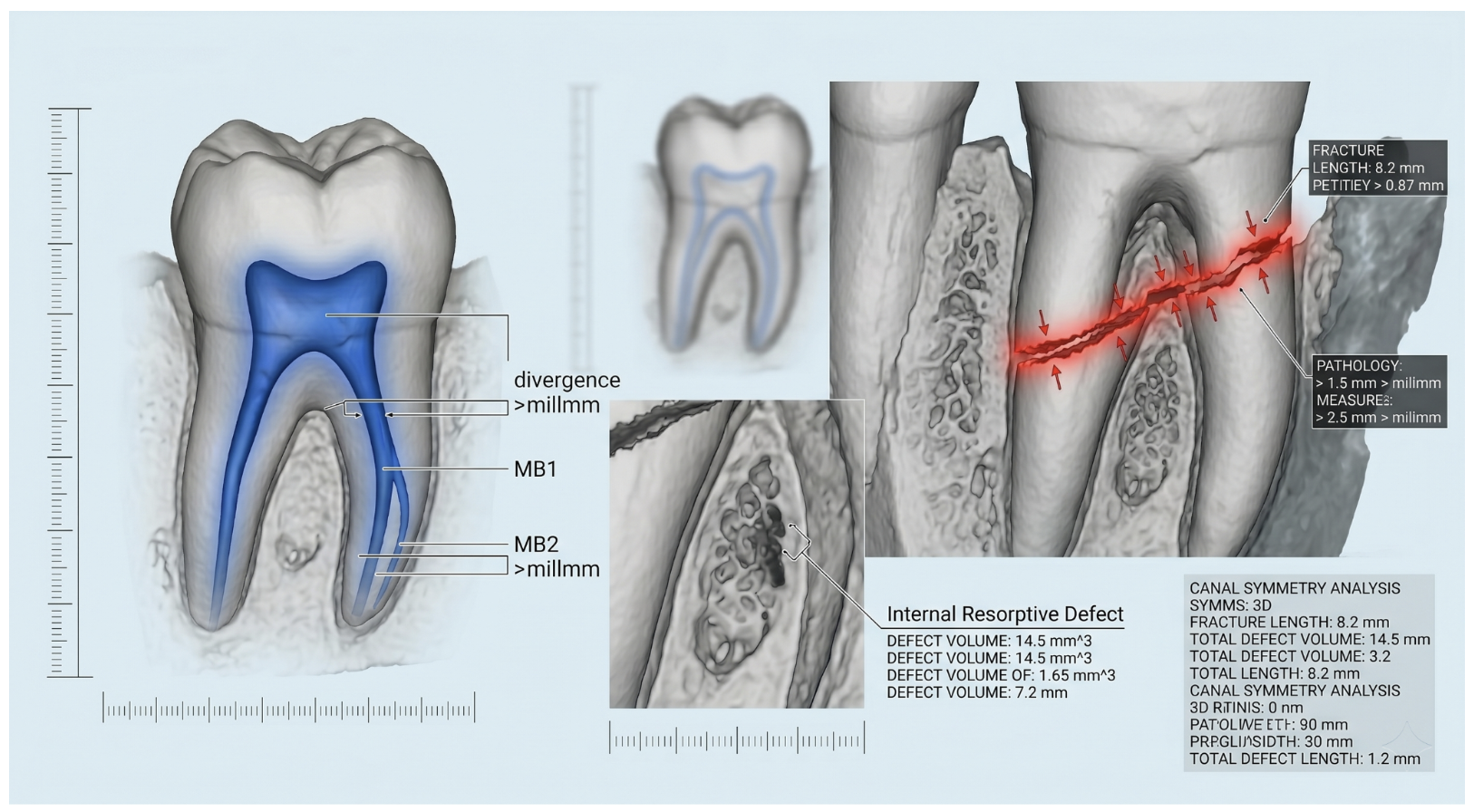
Root Anatomy
CBCT can reveal:
- Additional canals
- Complex root morphology
- Root fractures
- Resorptive defects
- Canal anatomy
This becomes particularly valuable in difficult endodontic cases.
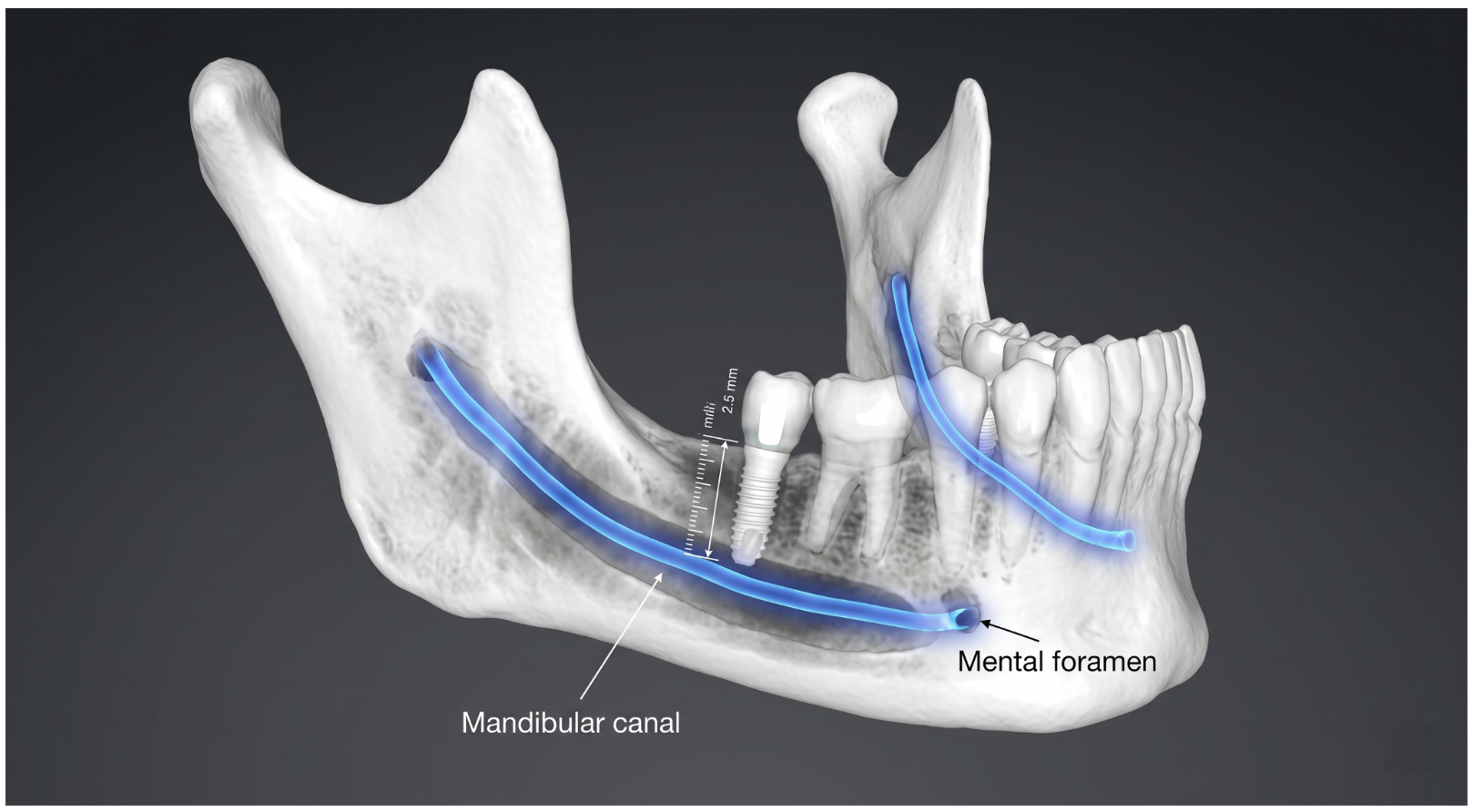
Neural Structures
CBCT allows direct visualization of:
- Inferior alveolar nerve
- Mandibular canal
- Mental foramen
- Neural pathways
Understanding nerve location improves safety during surgical procedures.
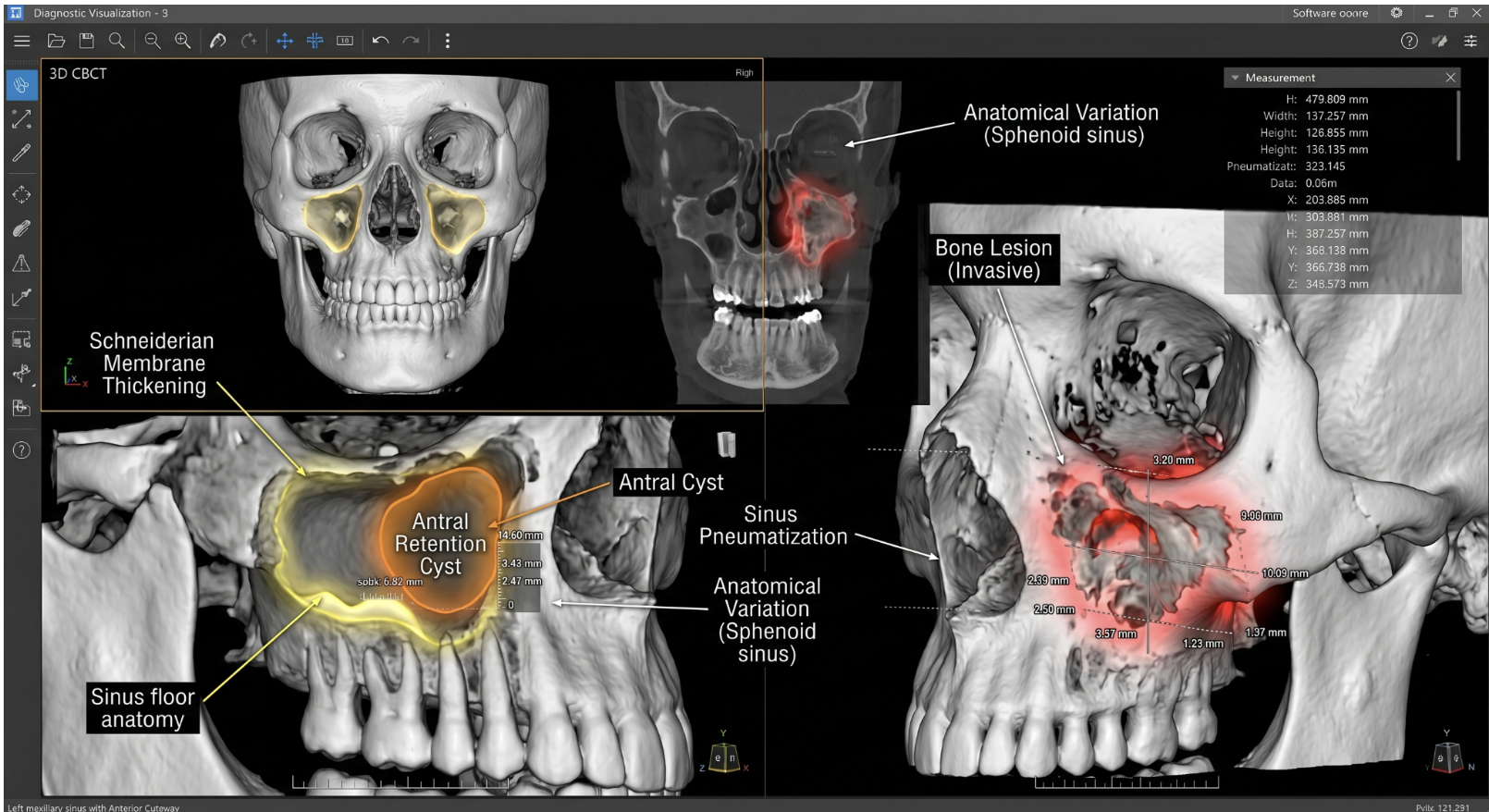
Sinus and Pathology Assessment
Clinicians can assess:
- Sinus floor anatomy
- Membrane conditions
- Anatomical variations
- Cysts
- Tumors
- Bone lesions
This level of detail frequently influences surgical planning and risk assessment.
Adoption of CBCT in Modern Dentistry
The use of CBCT continues to grow across dental specialties.
Current industry trends indicate:
- Approximately 60–70% of medium and large dental groups operate at least one in-house CBCT system
- Around 70–80% of implant-focused practices use CBCT as their default imaging modality for implant planning
This growth reflects increasing demand for precision-driven dentistry. However, increased availability does not mean routine use is appropriate. The purpose of CBCT is not to replace OPG. Its purpose is to answer clinical questions that panoramic imaging cannot answer adequately.
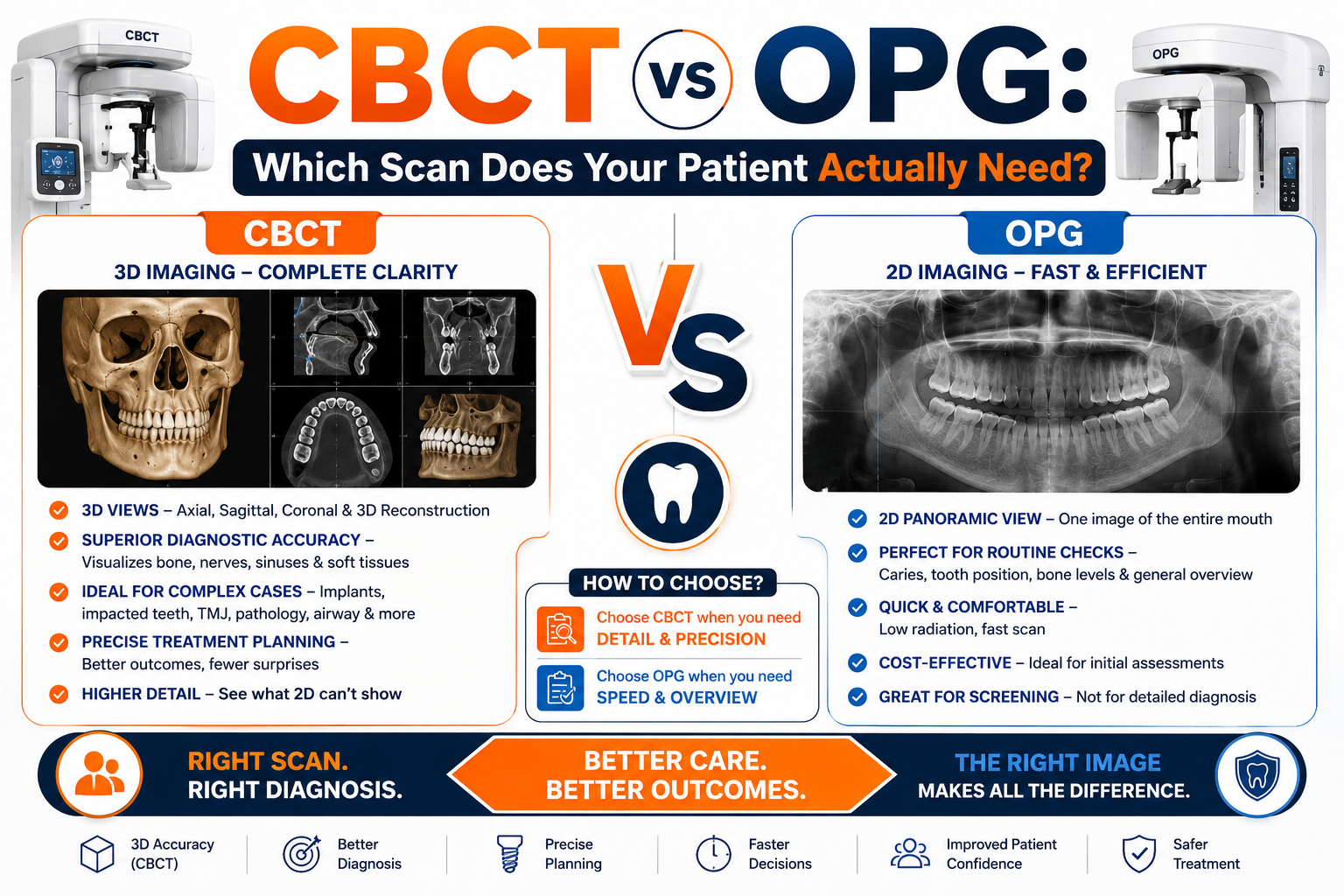
CBCT vs OPG: Side-by-Side Comparison
| Factor | OPG | CBCT |
| Image Type | 2D | 3D |
| Radiation Exposure | Lower | Higher |
| Cost | Lower | Higher |
| Screening | Excellent | Not Recommended |
| Implant Planning | Limited | Excellent |
| Endodontic Planning | Limited | Excellent |
| Impacted Teeth Evaluation | Basic | Precise |
| Fracture Assessment | Limited | Detailed |
| Surgical Planning | Limited | Comprehensive |
| Orthodontic Screening | Usually Sufficient | Selective Use |
| Anatomical Measurement | Approximate | Precise |
| Treatment Accuracy | Moderate | High |
Clinical Takeaway
The difference between OPG and CBCT can be summarized through the questions they answer.
OPG helps clinicians understand: “What is happening?”
CBCT helps clinicians understand: “Exactly where it is, how much is involved, and what structures are nearby?”
Both technologies remain important because they answer different clinical questions. One provides perspective. The other provides precision.
When Is OPG the Right Choice?
Despite the growing popularity of CBCT, most patients entering a dental clinic still do not require three-dimensional imaging. This is because many routine diagnostic questions can be answered effectively through panoramic radiography. OPG remains the preferred first-line imaging modality when clinicians need a broad overview of oral health rather than highly detailed anatomical measurements.
For general dental examinations, OPG helps assess the overall condition of the dentition, bone levels, impacted teeth, missing teeth, and obvious pathology in a single image. It is also widely used in orthodontics, where panoramic and cephalometric radiographs remain sufficient for most routine treatment planning. Similarly, for uncomplicated wisdom tooth assessment and general prosthodontic planning, panoramic imaging often provides all the information necessary for clinical decision-making.
The reason OPG continues to be so widely used is simple. It delivers:
- Broad anatomical visibility
- Lower radiation exposure
- Faster workflow
- Lower cost
- Effective screening capability
For routine diagnosis, that combination is difficult to beat.
When Does CBCT Become Essential?
CBCT becomes valuable when treatment success depends on understanding anatomy in three dimensions. At this stage, the clinician is no longer asking what is present but rather where it is located, how much anatomy is available, and what critical structures are nearby.
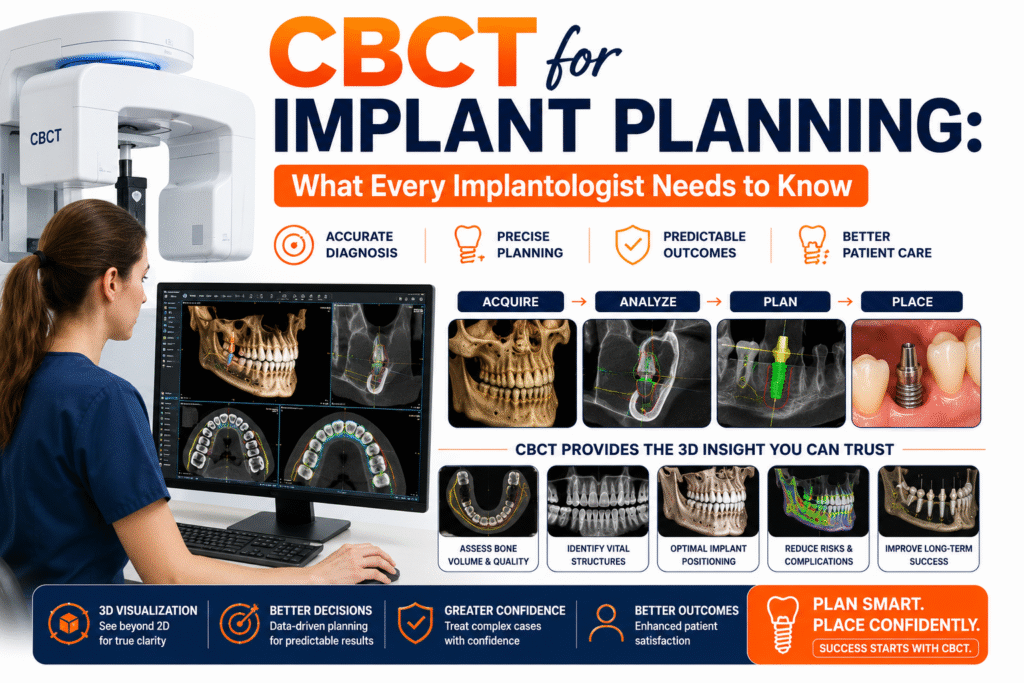
Implant Planning
Implant dentistry remains one of the strongest indications for CBCT imaging. Successful implant placement requires accurate assessment of:
- Bone height
- Bone width
- Bone morphology
- Nerve proximity
- Sinus anatomy
A panoramic image can provide an overview, but CBCT allows direct measurement and surgical planning. This level of precision explains why approximately 70–80% of implant-focused practices now use CBCT as their default imaging modality for implant planning.
Impacted Teeth Localization
When impacted teeth are positioned close to adjacent roots or neural structures, three-dimensional imaging becomes extremely useful. CBCT allows clinicians to determine:
- Exact tooth position
- Root angulation
- Buccal-lingual relationships
- Nerve proximity
- Cortical bone involvement
This improves surgical predictability and reduces the likelihood of unexpected findings during treatment.
Complex Endodontics
Most routine root canal treatments can be planned using conventional radiographs. However, CBCT becomes valuable when clinicians suspect:
- Missed canals
- Vertical root fractures
- Persistent infection
- Complex root anatomy
- Retreatment challenges
Because CBCT eliminates anatomical superimposition, it often reveals structures hidden on two-dimensional images.
Oral Surgery, Pathology, TMJ and Airway Assessment
Three-dimensional imaging is frequently indicated when evaluating:
- Cysts
- Tumors
- Jaw fractures
- Surgical extraction sites
- Bone defects
- TMJ abnormalities
- Airway dimensions
In these situations, treatment planning often depends on precise anatomical relationships that panoramic imaging cannot fully demonstrate.
Radiation Exposure
Radiation exposure is one of the most common concerns when comparing CBCT and OPG. The reality is that CBCT exposes patients to more radiation than panoramic imaging, but substantially less than conventional medical CT.
Current evidence suggests: CBCT generally exposes patients to approximately 2–10 times more radiation than OPG. However: CBCT delivers approximately 5–20 times less radiation than conventional medical CT scans
This is why CBCT is considered a moderate-dose imaging modality rather than a high-dose one. Modern systems continue to improve radiation efficiency through:
- Low-dose protocols
- Smaller field-of-view imaging
- Advanced reconstruction algorithms
- AI-assisted image optimization
Professional guidance from the American Academy of Oral and Maxillofacial Radiology and American Association of Endodontists consistently recommends using the smallest field of view necessary to answer the clinical question.
The principle remains simple: Order CBCT only when the additional information will influence diagnosis or treatment.
AI and the Future of Dental Imaging
The future of dental imaging is not about replacing OPG with CBCT. It is about combining advanced imaging, artificial intelligence, and radiologist expertise to improve diagnostic accuracy and workflow efficiency.
AI-Assisted OPG Reporting
Modern AI systems can assist with preliminary interpretation of panoramic radiographs by identifying potential abnormalities and highlighting regions that deserve closer review. At Nidaan Dental, AI-assisted OPG workflows support reporting through:
- Automated X-ray analysis
- Color-coded abnormality marking
- Structured report generation
- Faster preliminary review
This allows clinicians to identify suspicious findings more efficiently while ensuring every report undergoes professional radiologist validation.
AI-Assisted CBCT Reporting
CBCT generates large volumes of imaging data that require detailed interpretation. To improve consistency and efficiency, Nidaan uses AI-assisted tools to support:
- Report drafting
- Anatomical structuring
- Observation organization
- Workflow acceleration
The purpose is not automated diagnosis. Instead, AI helps radiologists prepare comprehensive reports more efficiently while reducing the risk of omissions. The final interpretation remains entirely radiologist-led.
This reflects the future of dental imaging: Technology enhances precision. Clinical expertise ensures accuracy.
Practical Decision Framework for Dentists
The simplest way to choose between OPG and CBCT is to focus on the clinical question.
Choose OPG When:
- Screening is the primary objective
- Diagnosis is straightforward
- No surgery is planned
- Radiation minimization is preferred
- A broad anatomical overview is sufficient
- Routine orthodontic evaluation is required
Choose CBCT When:
- Implant placement is planned
- Impacted teeth require localization
- Endodontic complexity exists
- Surgical planning is necessary
- Pathology assessment requires precision
- Conventional imaging is inconclusive
- TMJ or airway evaluation is required
A useful rule is: If three-dimensional information will change diagnosis, treatment planning, or risk assessment, CBCT is justified. If it does not, OPG is usually sufficient.
Expert Perspective
The debate is no longer whether CBCT provides more information than OPG. It clearly does. The more important question is whether that additional information improves patient care enough to justify its use.
This principle is reflected in the widely cited position statement from the American Academy of Oral and Maxillofacial Radiology and the American Association of Endodontists:
“CBCT should not be used as a screening tool; it should be prescribed only when the expected diagnostic benefit outweighs additional exposure and influences patient management.”
This recommendation remains one of the most important principles in evidence-based dental radiology today.
CBCT and OPG are not competing
CBCT and OPG are not competing technologies. They are complementary diagnostic tools designed for different clinical purposes. For routine examinations, orthodontic screening, referral imaging, and broad dental assessment, OPG continues to provide an efficient and cost-effective overview of oral health.
For implant planning, impacted teeth, complex endodontics, pathology assessment, surgical procedures, and advanced diagnostics, CBCT provides the anatomical precision required for safer and more predictable treatment outcomes.
Ultimately, successful imaging is not about choosing the most advanced technology available. It is about choosing the right scan for the right patient at the right time.
Explore Advanced CBCT and OPG Imaging Services
Whether you need a panoramic dental assessment or advanced three-dimensional imaging for treatment planning, choosing a radiology provider with experienced interpretation can significantly improve diagnostic confidence.
Explore Best CBCT and OPG Scan in Pune to learn more about advanced dental imaging services, radiologist-reviewed reporting, AI-assisted workflows, and comprehensive diagnostic support available through Nidaan Dental.
Frequently Asked Questions
Which is better: CBCT or OPG?
CBCT and OPG are designed for different clinical purposes, so neither scan is universally better than the other. The right choice depends on the diagnostic information needed and the complexity of the case.
An OPG (Orthopantomogram) is usually the preferred first-line imaging modality for routine dental examinations, orthodontic assessment, wisdom tooth evaluation, and general screening because it provides a broad overview of the teeth, jaws, and surrounding structures in a single image.
A CBCT (Cone Beam Computed Tomography) scan becomes the better option when treatment decisions require detailed three-dimensional information. This includes procedures such as dental implant planning, impacted tooth surgery, complex root canal treatment, pathology assessment, and oral surgery.
A simple way to remember the difference is: OPG provides the overview. CBCT provides the precision.
Is a CBCT scan necessary for dental implants?
In most modern implant workflows, CBCT is considered the preferred imaging modality because successful implant placement depends on accurate three-dimensional assessment of the jawbone and surrounding anatomy.
Before placing an implant, your dentist needs to evaluate:
- Bone height and width
- Bone density and morphology
- Location of the inferior alveolar nerve
- Position of the maxillary sinus
- Available space for implant placement
- Anatomical limitations that could affect treatment
An OPG can provide a useful overview, but it cannot accurately measure bone dimensions or show the exact spatial relationship between implants and vital structures.
This is why CBCT has become the standard imaging tool in many implant-focused practices. By improving treatment planning accuracy, it helps reduce complications and contributes to more predictable implant outcomes.
Can an OPG scan detect impacted wisdom teeth?
Yes. An OPG scan is highly effective for identifying impacted wisdom teeth and remains one of the most commonly used imaging methods for third molar assessment.
The scan can help dentists evaluate:
- Whether the tooth is impacted
- Direction and angulation of eruption
- Available space within the jaw
- Relationship with adjacent teeth
- General root development
In many cases, this information is sufficient to make treatment decisions.
However, if the roots appear close to the inferior alveolar nerve or the anatomy appears unusually complex, your dentist may recommend a CBCT scan. CBCT can provide precise three-dimensional information about nerve proximity and surgical risk, helping improve treatment safety.
Why do dentists still use OPG when CBCT technology is available?
Although CBCT provides more detailed anatomical information, most dental patients do not require three-dimensional imaging for routine care.
Dentists continue to use OPG because it offers several important advantages:
- Lower radiation exposure
- Faster image acquisition
- Lower cost
- Broad anatomical coverage
- Efficient screening capability
For routine examinations, orthodontic evaluations, referral imaging, and general diagnosis, panoramic imaging often provides all the information necessary to make informed clinical decisions.
In fact, many treatment plans begin with an OPG and only progress to CBCT if additional anatomical detail becomes necessary. The goal is not to use the most advanced scan available. The goal is to use the scan that answers the clinical question effectively and responsibly.
Does a CBCT scan expose patients to more radiation than an OPG?
Yes. CBCT generally exposes patients to more radiation than a panoramic OPG scan because it captures detailed three-dimensional imaging data.
However, context is important. While CBCT typically involves higher radiation exposure than OPG, it still exposes patients to significantly less radiation than a conventional medical CT scan.
Modern CBCT systems have also become more dose-efficient through:
- Low-dose scanning protocols
- Small field-of-view imaging
- Improved detector technology
- AI-assisted image reconstruction
Dentists follow radiation protection principles such as ALARA (As Low As Reasonably Achievable), meaning CBCT is only recommended when the additional information is expected to influence diagnosis or treatment planning.
When clinically justified, the diagnostic benefits of CBCT usually outweigh the small increase in radiation exposure.
What dental conditions are best evaluated with CBCT?
CBCT is most valuable when clinicians require accurate three-dimensional visualization of anatomical structures that cannot be adequately assessed using conventional radiographs.
Common indications include:
- Dental implant planning
- Impacted teeth localization
- Complex root canal cases
- Persistent endodontic infections
- Vertical root fractures
- Jaw fractures
- Bone defects
- Cysts and tumors
- Temporomandibular joint (TMJ) assessment
- Airway analysis
- Oral and maxillofacial surgical planning
In these situations, CBCT often provides information that directly influences treatment decisions, surgical safety, and long-term outcomes.
Can CBCT detect problems that an OPG scan may miss?
Yes. One of the major advantages of CBCT is its ability to eliminate anatomical overlap and reveal structures that may not be clearly visible on two-dimensional panoramic images.
Depending on the case, CBCT may identify:
- Hidden root fractures
- Additional root canals
- Bone defects
- Early pathology
- Precise nerve pathways
- Impacted tooth relationships
- Sinus abnormalities
- Extent of cysts and lesions
- Complex root anatomy
Because clinicians can examine anatomy in multiple planes, CBCT often improves diagnostic confidence when conventional imaging provides incomplete information.
This additional level of detail is one of the reasons CBCT has become increasingly important in implantology, endodontics, and oral surgery.
How is artificial intelligence (AI) being used in dental imaging?
Artificial intelligence is increasingly being integrated into dental imaging workflows to improve efficiency, consistency, and diagnostic support.
AI can assist with:
- Identifying potential abnormalities
- Highlighting suspicious findings
- Supporting image interpretation
- Organizing radiology reports
- Improving workflow efficiency
- Assisting with image measurements
At Nidaan, AI is used as a support tool rather than a replacement for clinical expertise.
For OPG imaging, AI-assisted systems help by:
- Generating structured reports
- Highlighting abnormalities using color-coded markers
- Supporting preliminary review workflows
For CBCT imaging, AI assists with:
- Report drafting
- Anatomical segmentation
- Structured documentation
- Workflow acceleration
Importantly, all findings continue to be reviewed and validated by qualified radiologists before reports are finalized. Technology improves efficiency, while expert interpretation ensures accuracy.
Is CBCT safe for children and younger patients?
CBCT can be safely used in children when there is a valid clinical indication and the expected diagnostic benefit outweighs the additional radiation exposure.
Modern pediatric imaging protocols focus on minimizing exposure through:
- Low-dose acquisition modes
- Reduced scan volume
- Smaller field-of-view selection
- Optimized imaging parameters
Examples where CBCT may be appropriate in younger patients include:
- Impacted teeth assessment
- Complex orthodontic planning
- Craniofacial anomalies
- Airway evaluation
- Certain surgical cases
Professional guidelines recommend that CBCT should never be used routinely in children and should only be prescribed when the additional information is expected to influence treatment planning or outcomes.
When should a dentist order a CBCT scan instead of an OPG?
A dentist should consider CBCT when the clinical situation requires information that cannot be accurately obtained through conventional panoramic imaging.
CBCT is typically recommended when:
- Implant placement is planned
- Impacted teeth require precise localization
- Complex root canal anatomy is suspected
- Surgical treatment is being considered
- Pathology requires detailed assessment
- Nerve relationships need evaluation
- Conventional imaging is inconclusive
- TMJ or airway analysis is required
A useful clinical rule is: If three-dimensional information could change the diagnosis, treatment plan, surgical approach, or risk assessment, CBCT is usually justified. If panoramic imaging already provides sufficient information for decision-making, OPG remains the more appropriate first-line choice.
The best imaging decision is not about choosing the newest technology, it is about selecting the scan that provides the right information for the right patient at the right time.