TL;DR
- CBCT is the preferred imaging modality for dental implant planning because it provides accurate three-dimensional visualization of implant sites.
- Unlike panoramic radiographs (OPG), CBCT allows precise measurement of bone height, bone width, ridge morphology, and critical anatomical structures.
- Approximately 75–80% of implant sites are now planned using CBCT-derived 3D workflows and guided surgery systems.
- Around 85–90% of advanced implant centers routinely use CBCT-based planning platforms before implant placement.
- CBCT-guided planning has been associated with approximately 30% fewer nerve and sinus-related complications compared with traditional two-dimensional workflows.
- Modern guided surgery systems rely on CBCT-derived DICOM datasets for virtual planning and surgical guide fabrication.
- Low-dose CBCT protocols now account for approximately 60–70% of implant-planning scans, supporting safer imaging while maintaining diagnostic quality.
Modern implantology has moved far beyond estimating implant positions from two-dimensional radiographs. Today, successful implant placement depends on understanding bone anatomy, nerve pathways, sinus relationships, and restorative requirements in three dimensions before surgery begins.
The biggest shift is not technological. It is clinical. Implant planning is no longer based primarily on estimation. It is based on visualization, measurement, and predictability.
Direct Answer
CBCT (Cone Beam Computed Tomography) is the preferred imaging modality for dental implant planning because it provides accurate three-dimensional visualization of bone volume, ridge dimensions, nerve pathways, sinus anatomy, and implant site characteristics. Unlike OPG, which provides only a two-dimensional overview, CBCT allows clinicians to measure implant positions precisely, evaluate anatomical limitations, plan guided surgery, and reduce surgical risks before treatment begins.
In practical terms: OPG helps identify whether implant treatment may be possible. CBCT helps determine exactly how implant treatment should be performed. That difference is what makes CBCT a cornerstone of modern implant dentistry.
Why Has CBCT Become the Foundation of Modern Implant Planning?
Not long ago, implant placement depended heavily on clinical judgment, panoramic radiographs, and intraoperative decision-making. Experienced clinicians achieved excellent results, but treatment planning often involved a greater degree of interpretation because key anatomical structures could not always be visualized clearly.
Today, patient expectations are different.
Your patients expect:
- predictable outcomes
- shorter treatment times
- minimally invasive procedures
- digitally planned treatment
- fewer complications
At the same time, implantologists are increasingly adopting restorative-driven workflows where implant placement begins with the final prosthetic outcome in mind rather than simply placing an implant where bone appears available.
This evolution has made three-dimensional imaging indispensable.
Recent industry data demonstrates how rapidly implant workflows have shifted toward CBCT-based planning. Approximately 75–80% of implant sites are now planned using CBCT-derived three-dimensional workflows, while 85–90% of advanced implant centers routinely integrate CBCT planning software before surgery.
These numbers reflect a broader reality. Modern implantology is becoming increasingly digital, guided, and data-driven.
As contemporary implantology reviews note:
“CBCT-based 3D imaging allows measurements in dimensions not previously available, improving surgical predictability.”
That improvement in predictability is precisely why CBCT has become such a critical part of implant planning.
What Makes CBCT Essential for Dental Implant Planning?
The real value of CBCT becomes clear when you compare what clinicians need for implant placement with what conventional radiographs can actually provide.
The Limitation of Two-Dimensional Imaging
Panoramic imaging remains useful for screening and preliminary assessment. It can help visualize teeth, major anatomical landmarks, and general bone levels. However, implant treatment requires significantly more information than routine diagnosis.
For example, an OPG may suggest that adequate bone exists in a region.
What it cannot reliably determine is:
- true buccolingual bone width
- cortical thickness
- ridge contour
- exact nerve location
- precise sinus relationships
- implant angulation requirements
These details matter because implant success is measured in millimeters. A small miscalculation can increase the risk of:
- nerve injury
- sinus perforation
- implant instability
- prosthetic compromise
- esthetic failure
The challenge is not seeing anatomy. The challenge is understanding anatomy accurately.
How CBCT Changes the Planning Process
CBCT transforms implant planning by providing a volumetric dataset that can be viewed from sagittal, axial, and coronal perspectives. Instead of interpreting anatomy from a flat image, you can evaluate structures exactly as they exist.
This allows detailed assessment of:
Bone Quantity
Successful implant placement starts with understanding available bone volume. CBCT enables accurate measurement of:
- vertical bone height
- horizontal ridge width
- ridge morphology
- implant envelope dimensions
Recent comparative studies found CBCT measurements to be approximately 0.76 mm more accurate than panoramic measurements, with panoramic radiographs frequently overestimating available bone.
While less than a millimeter may appear insignificant, it can be the difference between predictable implant placement and surgical complications.
Critical Anatomical Structures
One of the greatest strengths of CBCT is its ability to clearly identify anatomical landmarks that directly influence surgical safety.
These include:
- inferior alveolar nerve
- mental foramen
- incisive canal
- maxillary sinus floor
- nasal cavity boundaries
- adjacent root structures
By visualizing these structures in three dimensions, clinicians can establish safe surgical zones before treatment begins rather than discovering limitations during surgery.
Bone Morphology and Quality
Implant success depends not only on the amount of bone available but also on its quality and architecture. CBCT assists clinicians in evaluating:
- cortical integrity
- trabecular patterns
- ridge shape
- augmentation requirements
- implant stability potential
This additional layer of information often influences implant selection and loading protocols.
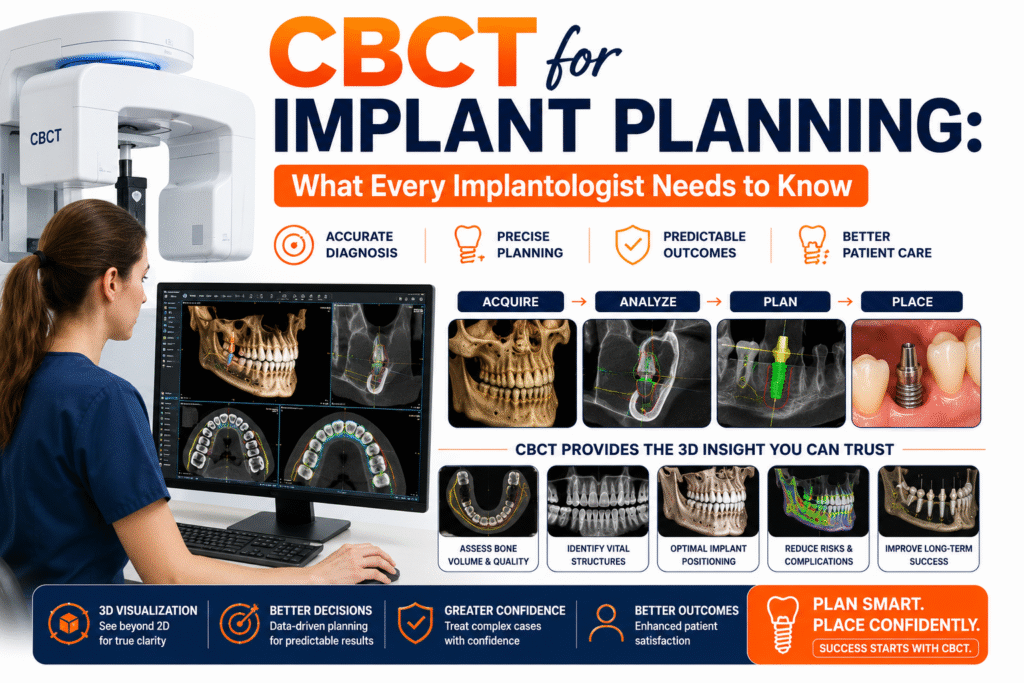
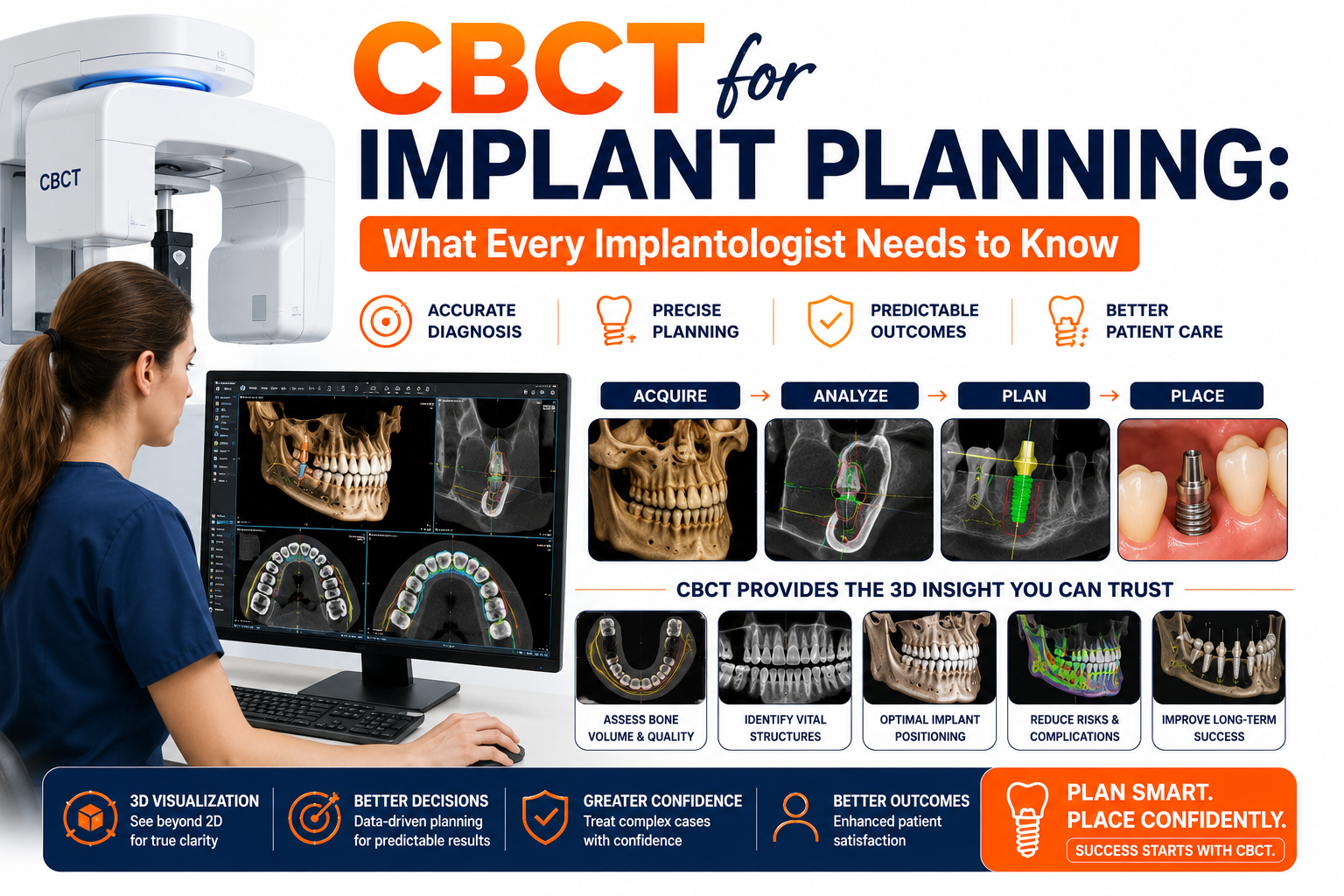
Step-by-Step CBCT Implant Planning Workflow
One reason CBCT has become central to implant dentistry is that it integrates seamlessly into modern digital workflows. Rather than serving as a standalone imaging tool, it functions as the foundation of the entire treatment-planning process.
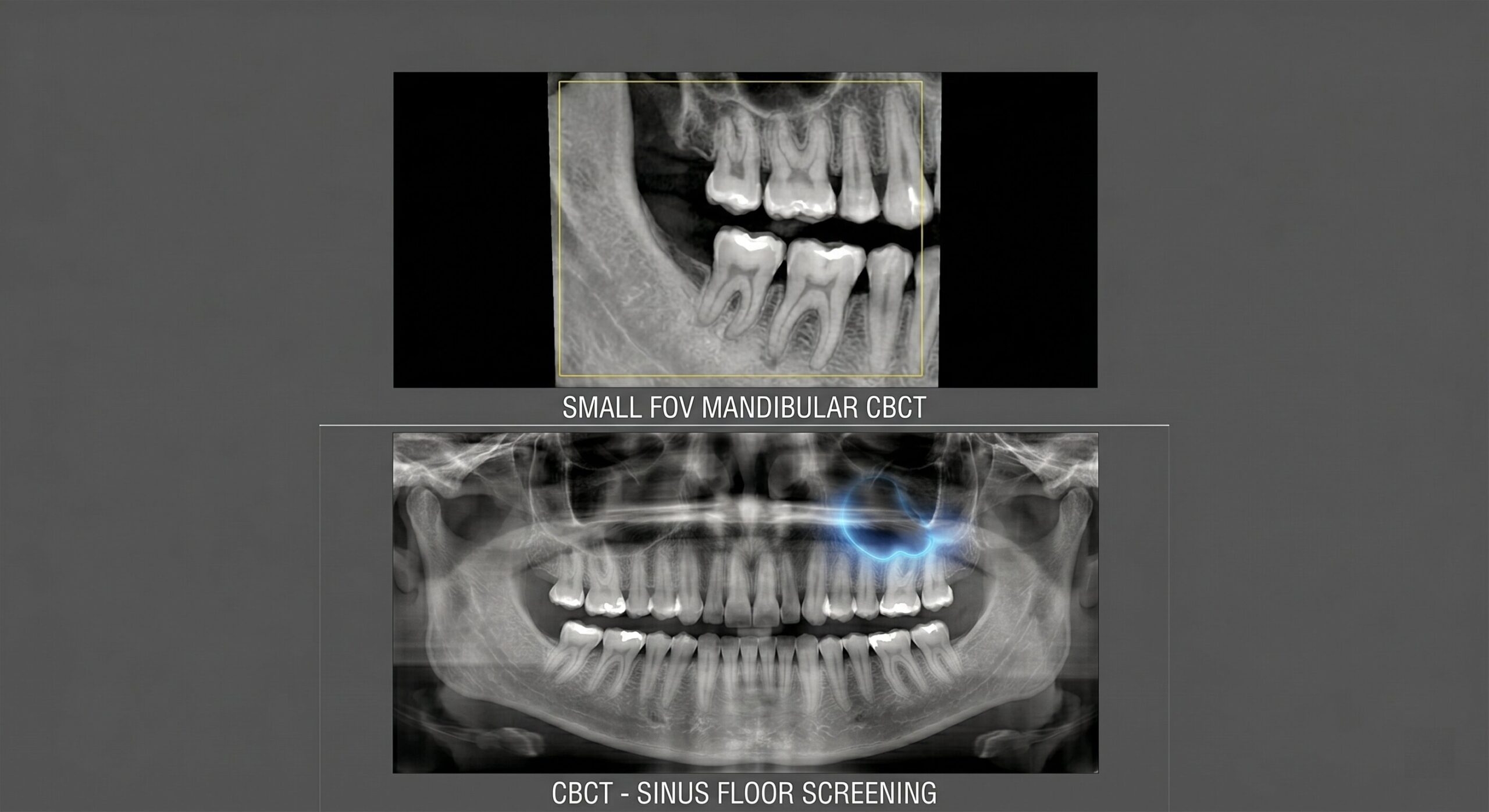
Step 1: Acquire the Appropriate CBCT Scan
The process begins with image acquisition.
Current guidelines emphasize selecting:
- the smallest field of view necessary
- implant-specific imaging protocols
- optimized low-dose settings
- appropriate exposure parameters
The objective is always to obtain diagnostic-quality images while following the ALARA principle (As Low As Reasonably Achievable). Interestingly, approximately 60–70% of implant-planning scans now use low-dose CBCT protocols, reflecting growing emphasis on radiation optimization.

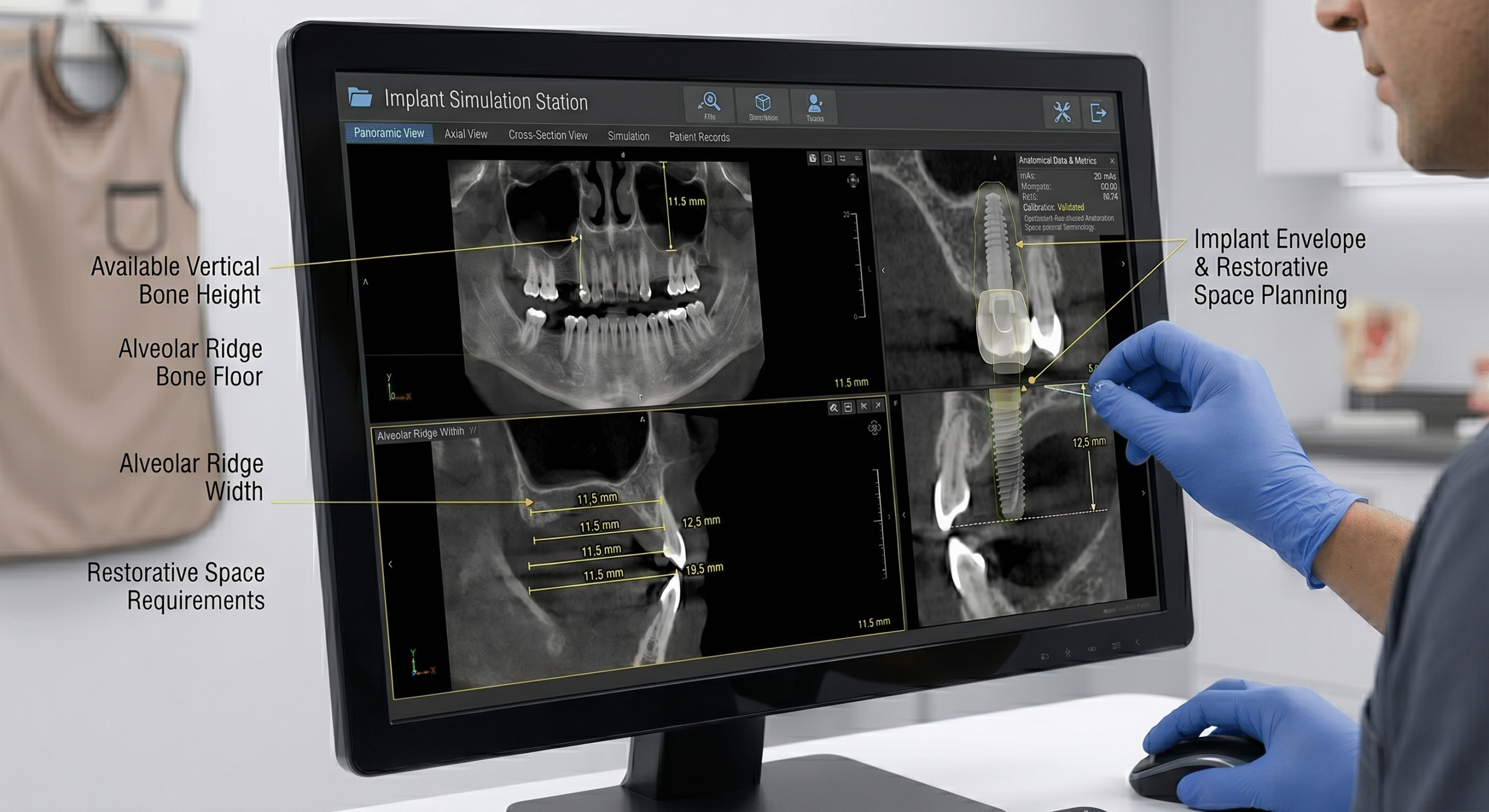
Step 2: Analyze Bone Dimensions
Once imaging is completed, clinicians evaluate the implant site in detail.
Measurements typically include:
- available vertical bone height
- ridge width
- implant envelope dimensions
- restorative space requirements
This stage establishes which implant dimensions are feasible before treatment begins.
Step 3: Map Anatomical Risk Areas
The next step focuses on identifying structures that could influence implant placement. These include:
- mandibular canal
- mental foramen
- sinus floor
- adjacent roots
- cortical boundaries
Accurate mapping reduces the likelihood of complications and improves surgical confidence.

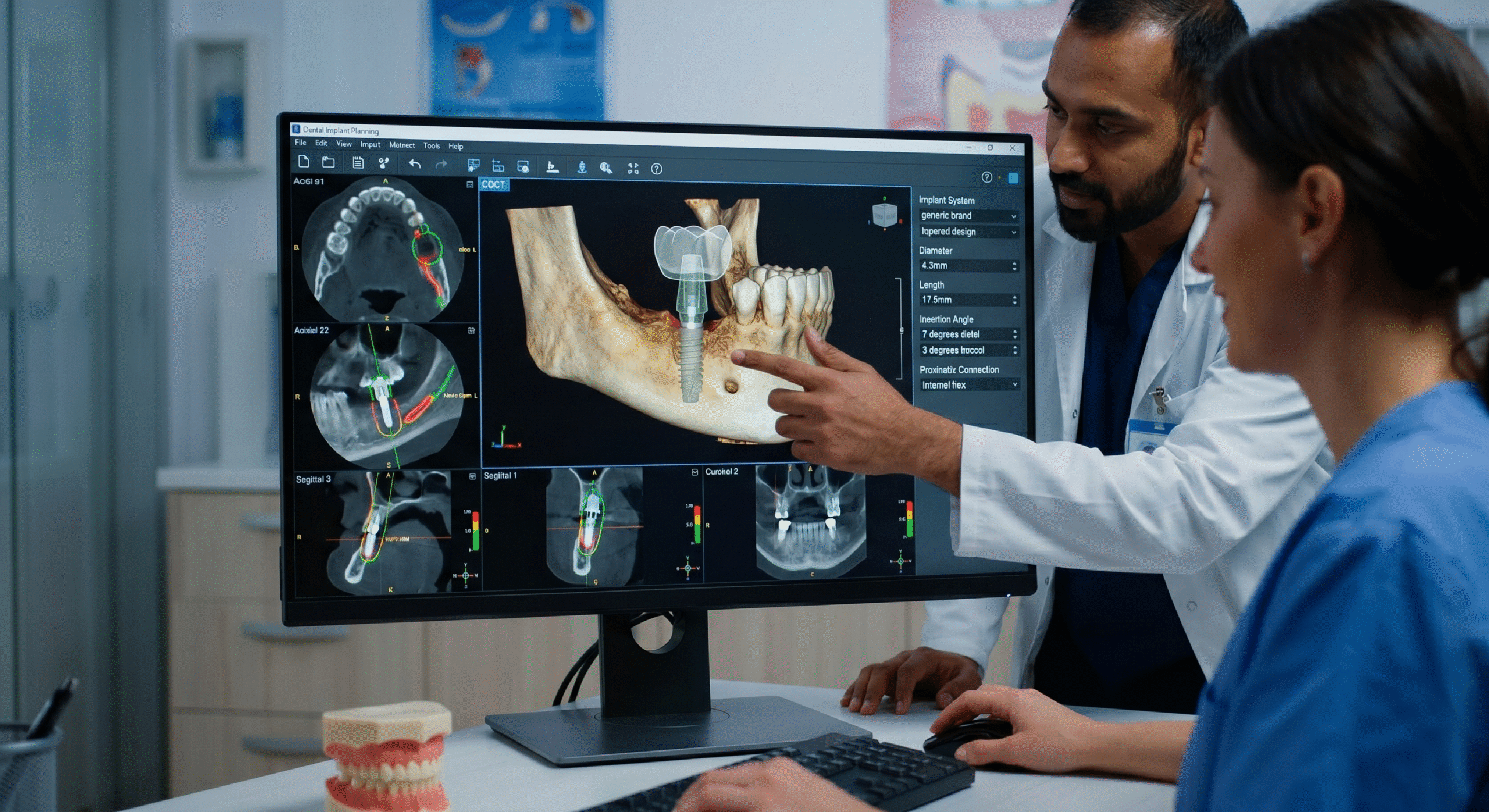
Step 4: Virtually Position the Implant
Modern planning software allows clinicians to simulate implant placement digitally before entering the surgical operation.
This enables selection of:
- implant diameter
- implant length
- insertion angle
- restorative emergence profile
- prosthetic positioning
Instead of making decisions during surgery, treatment planning happens beforehand in a controlled environment.
Step 5: Integrate Guided Surgery
Once planning is finalized, the CBCT dataset can be combined with intraoral scans and CAD software to produce surgical guides. This transforms the workflow from: Estimation → Placement
Into: Planning → Verification → Guided Execution. That shift represents one of the biggest advancements in contemporary implantology.
Implant Cases Where CBCT Becomes Essential
Although CBCT offers advantages in nearly every implant case, certain clinical situations benefit particularly from three-dimensional planning.
Posterior Mandible Cases
The relationship between implant sites and the inferior alveolar nerve can significantly influence treatment safety. CBCT enables precise nerve mapping, helping clinicians determine safe implant dimensions and positioning before osteotomy preparation begins.
Sinus Proximity Cases
When implants are planned in the posterior maxilla, sinus anatomy becomes critically important.
CBCT allows evaluation of:
- sinus floor position
- residual bone height
- sinus septa
- membrane anatomy
- augmentation requirements
This information is essential for predictable sinus lift planning and implant placement.
Atrophic Ridge Cases
Patients with significant ridge resorption often require complex decision-making regarding grafting procedures, implant selection, and surgical limitations.
Three-dimensional imaging provides a far more accurate assessment of available bone than conventional radiography alone.
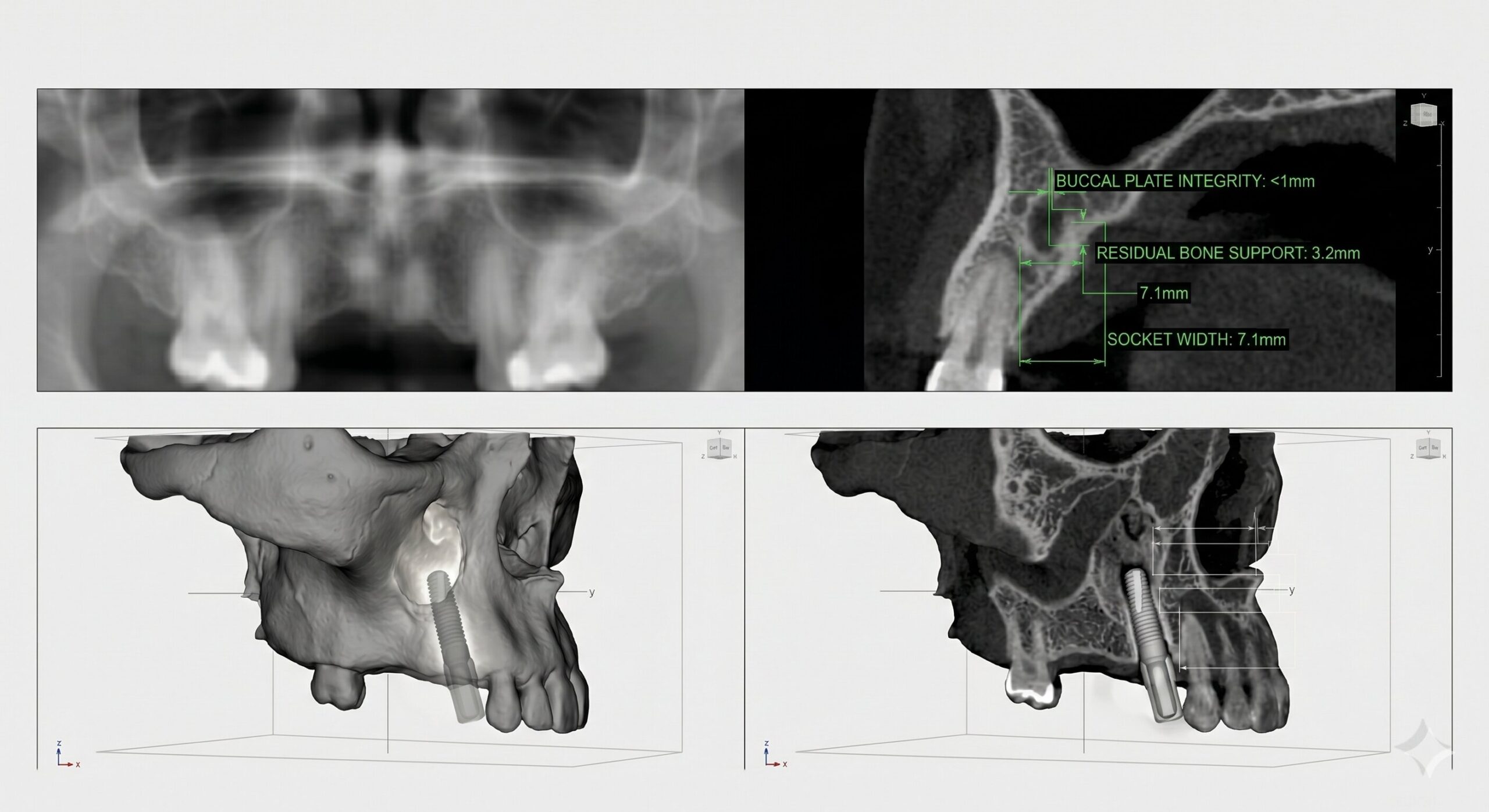
Immediate Implant Placement
Immediate placement protocols require a detailed understanding of:
- socket morphology
- buccal plate integrity
- residual bone support
- anatomical limitations
These assessments are significantly more predictable when performed using CBCT imaging.
![]()
![]()
CBCT vs OPG for Implant Planning: Which Imaging Method Provides Better Implant Data?
Both OPG and CBCT have a place in implant dentistry, but they serve very different purposes.
Panoramic radiography is valuable for initial screening because it provides a broad overview of the jaws, remaining dentition, and major anatomical landmarks. It can help identify whether implant treatment may be possible and highlight obvious anatomical concerns.
However, implant planning requires decisions based on millimeter-level precision.
Clinicians must determine:
- Exact implant dimensions
- Available bone volume
- Ridge morphology
- Nerve proximity
- Sinus relationships
- Implant angulation
- Prosthetic positioning
These variables cannot be assessed reliably through two-dimensional imaging alone. This is why CBCT has become the preferred imaging modality for modern implant planning.
| Planning Factor | OPG | CBCT |
| Bone Height Assessment | Moderate Accuracy | Highly Accurate |
| Bone Width Measurement | Not Reliable | Accurate |
| Ridge Morphology Analysis | Limited | Comprehensive |
| Nerve Mapping | Limited | Excellent |
| Sinus Assessment | Limited | Excellent |
| Implant Simulation | Not Possible | Fully Supported |
| Guided Surgery Integration | No | Yes |
| Surgical Predictability | Moderate | High |
| Restorative Planning | Basic | Advanced |
| Anatomical Precision | Moderate | High |
The difference becomes particularly important in complex cases.
Research cited in your source material found that CBCT measurements of bone dimensions were approximately 0.76 mm more accurate than panoramic measurements, while panoramic radiographs frequently overestimated available bone volume.
More importantly, CBCT evaluation altered the final implant diameter or implant length selection in approximately 10–12% of implant sites, while 60–65% of sites initially planned using OPG required modification after CBCT assessment.
The clinical implication is clear: A treatment plan based solely on panoramic imaging may not always represent the patient’s true anatomical situation.
How CBCT Improves Implant Success and Predictability
Successful implant treatment depends on reducing uncertainty before surgery begins. Every unknown variable increases risk. Every accurately identified anatomical detail improves predictability. This is where CBCT creates its greatest clinical value.
Better Implant Site Selection
Three-dimensional imaging allows clinicians to identify anatomical limitations that may not be visible on conventional radiographs.
Examples include:
- Hidden ridge deficiencies
- Buccal plate defects
- Lingual undercuts
- Narrow ridge morphology
- Anatomical concavities
Identifying these limitations before surgery allows treatment plans to be modified proactively rather than reactively. As a result, implant selection becomes more accurate and treatment decisions become more predictable.
Fewer Surgical Surprises
One of the most important benefits of CBCT planning is reducing unexpected findings during surgery. When anatomy is visualized clearly before treatment, clinicians can avoid complications such as:
- Inferior alveolar nerve injury
- Mental nerve injury
- Sinus perforation
- Cortical plate perforation
- Inadequate implant positioning
- Incorrect implant angulation
Recent evidence suggests CBCT-guided planning is associated with approximately 30% fewer nerve-related and sinus-related complications compared with traditional two-dimensional workflows.
For implantologists, that improvement directly affects patient safety and treatment confidence.
Improved Prosthetically Driven Planning
Modern implantology increasingly follows a restorative-driven philosophy. Rather than placing implants wherever bone appears available, clinicians begin with the intended restoration and work backward toward implant positioning.
CBCT supports this approach by allowing evaluation of:
- Prosthetic emergence profile
- Implant angulation
- Restorative space
- Bone availability
- Anatomical limitations
The result is improved harmony between surgery and prosthetic rehabilitation. This often leads to better:
- Esthetics
- Function
- Occlusal relationships
- Long-term maintenance
Because successful implants are not judged solely by osseointegration. They are judged by restorative outcomes.
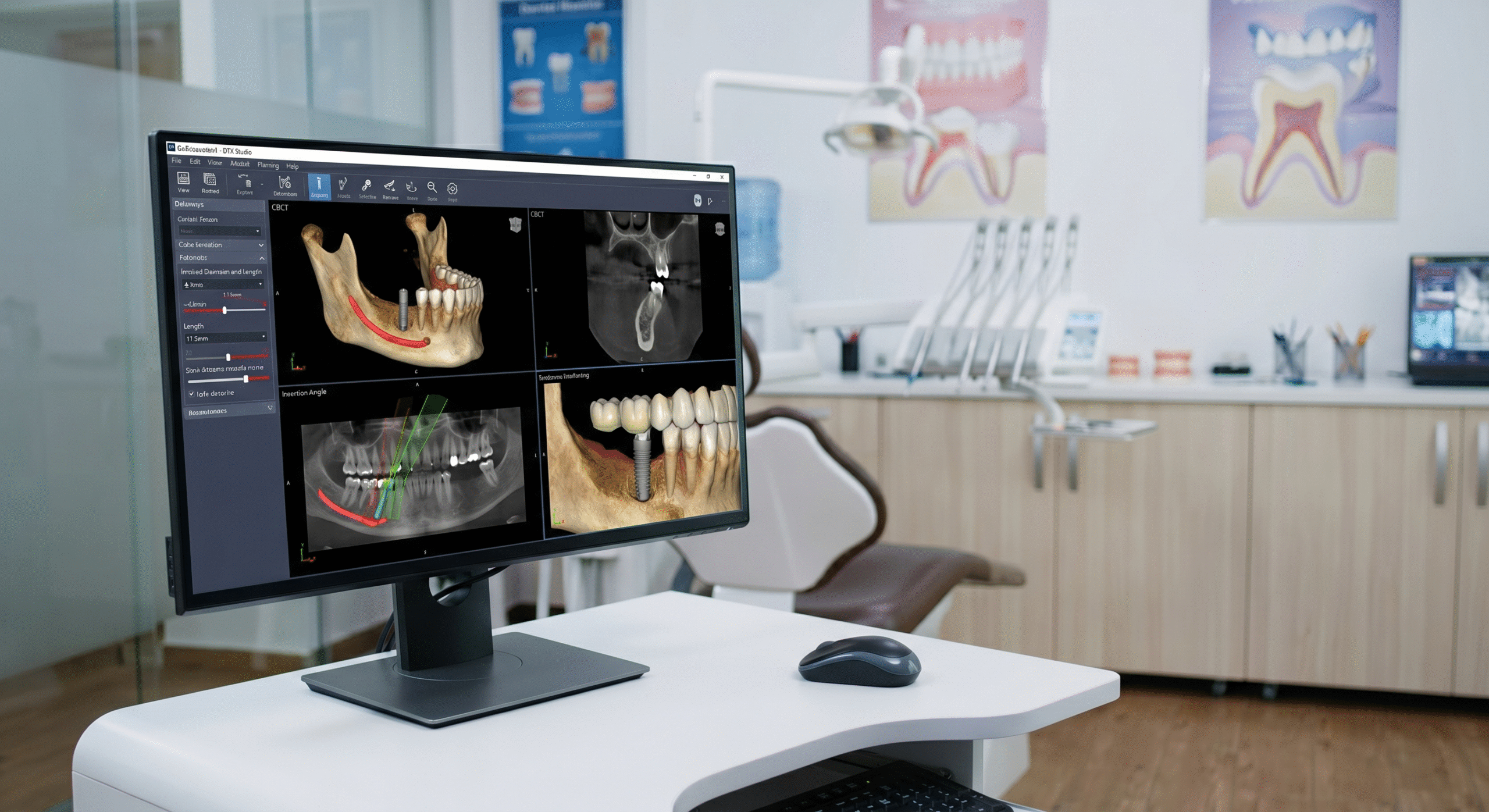
Guided Surgery and Digital Implant Workflows
Perhaps the biggest reason CBCT has become indispensable is its role in digital implant dentistry. The modern implant workflow is increasingly built around a fully digital planning environment.
Instead of making surgical decisions intraoperatively, clinicians can complete much of the planning process before the patient enters the operatory.
The Modern Digital Workflow
Today’s implant workflow often combines:
Intraoral Scanning
Digital capture of teeth and soft tissue anatomy.
CBCT Imaging
Three-dimensional visualization of bone and anatomical structures.
Implant Planning Software
Virtual implant placement and restorative simulation.
Surgical Guide Design
Translation of virtual planning into physical surgical guides.
Guided Implant Placement
Precise execution of the treatment plan.
Within this workflow, CBCT functions as the anatomical reference framework upon which every planning decision is based. Without accurate three-dimensional imaging, guided surgery simply cannot function as intended.
Why Guided Surgery Depends on CBCT
Guided surgery requires clinicians to know exactly:
- Where implants should be placed
- What angle they should follow
- How close anatomical structures are
- How much bone is available
- Whether grafting is required
These measurements are derived directly from CBCT datasets. The scan essentially becomes the digital blueprint of the surgical procedure.
Industry surveys cited in your source indicate approximately 40–50% of guided implant procedures in large group practices now operate through fully digital workflows centered around CBCT imaging. This trend continues to accelerate as digital dentistry becomes more mainstream.
Low-Dose CBCT and Radiation Considerations
Radiation exposure remains one of the most common concerns associated with CBCT imaging. Fortunately, implant-planning protocols have evolved significantly over the last decade. Modern systems now prioritize both diagnostic quality and radiation optimization.
Today many implant-focused protocols utilize:
- Small field-of-view imaging
- Low-dose acquisition settings
- Metal artifact reduction
- AI-assisted reconstruction algorithms
- Optimized exposure parameters
According to recent data, approximately 60–70% of implant-planning CBCT scans now use low-dose imaging protocols.
Research also demonstrates that low-dose CBCT protocols can maintain clinically acceptable diagnostic performance for implant planning while reducing patient exposure.
The principle remains straightforward: Use the lowest radiation dose capable of answering the clinical question. When implant placement depends on accurate anatomical information, the diagnostic benefits frequently outweigh the modest increase in exposure compared with panoramic imaging.
How AI Is Transforming CBCT Implant Planning
Artificial intelligence is beginning to influence implant workflows in ways that extend beyond simple image interpretation. Rather than replacing clinicians, AI is increasingly being used to improve planning efficiency and reporting consistency.
Modern systems can assist with:
- Automatic nerve tracing
- Anatomical landmark detection
- Sinus segmentation
- Implant site measurements
- Treatment simulation support
- Structured reporting workflows
These capabilities help reduce repetitive manual tasks and allow clinicians to focus more attention on treatment planning and decision-making.
How Nidaan Supports Implant Planning Workflows
At Nidaan Dental, AI is used as a clinical support system rather than an autonomous diagnostic tool.
For CBCT studies, AI-assisted workflows help:
- Draft structured reports
- Organize anatomical observations
- Improve reporting consistency
- Accelerate workflow efficiency
Every report remains subject to radiologist review and validation before finalization. This approach reflects a practical reality of modern imaging: Technology improves speed and consistency. Expert interpretation ensures clinical reliability.
Practical Decision Framework for Implantologists
CBCT should be strongly considered whenever implant treatment depends on precise anatomical information.
CBCT Is Recommended When:
- Implant placement is planned
- Bone dimensions influence treatment decisions
- Guided surgery workflows are being used
- Nerve pathways require evaluation
- Sinus proximity may affect implant positioning
- Immediate placement protocols are considered
- Multiple implants or full-arch rehabilitation is planned
- Significant ridge resorption exists
CBCT Becomes Particularly Valuable For:
- Posterior mandible implants
- Posterior maxillary implants
- Sinus lift procedures
- Atrophic ridges
- Full-arch restorations
- Immediate implant placement
- Esthetic zone rehabilitation
A useful clinical rule is: If implant positioning, surgical safety, restorative outcomes, or anatomical limitations depend on three-dimensional information, CBCT should be part of the planning process.
Expert Perspective
The role of CBCT in implantology is now supported by substantial clinical evidence and professional guidance.
As summarized in contemporary implant literature:
“CBCT could be justified for presurgical diagnosis, preoperative planning, and peroperative transfer for oral implant rehabilitation.”
This statement captures the evolution of implant dentistry. CBCT is no longer simply an imaging option. It has become an integral component of modern implant planning.
Dental implant success begins long before
Dental implant success begins long before the surgical appointment. It begins with planning.
CBCT has transformed implant dentistry by providing accurate three-dimensional information about bone volume, ridge morphology, nerve pathways, sinus anatomy, and implant site characteristics. Compared with traditional panoramic imaging, CBCT improves measurement accuracy, supports guided surgery workflows, reduces complications, and enhances restorative predictability.
As implant dentistry continues moving toward digital, guided, and restorative-driven workflows, CBCT is no longer just an imaging modality. It is the foundation upon which predictable implant treatment is built.
Advance Your Implant Planning with Accurate 3D Imaging
Whether you are planning a single implant, evaluating sinus proximity, performing immediate implant placement, or managing a complex full-arch rehabilitation, accurate imaging is the first step toward predictable outcomes.
Explore Best CBCT and OPG Scan in Pune to learn how advanced CBCT imaging, radiologist-reviewed reporting, and structured diagnostic workflows can support safer implant planning, improved surgical precision, and more confident treatment decisions.
Frequently Asked Questions
Why is CBCT considered the gold standard for dental implant planning?
CBCT is widely considered the preferred imaging modality for implant planning because it provides accurate three-dimensional visualization of the implant site before surgery begins. Unlike traditional panoramic radiographs, which show anatomy in only two dimensions, CBCT allows implantologists to evaluate bone height, bone width, ridge morphology, nerve pathways, sinus anatomy, and surrounding structures from multiple angles.
This level of detail helps clinicians answer critical questions before placing an implant:
- Is there enough bone available?
- How close is the implant site to the inferior alveolar nerve?
- Is sinus augmentation required?
- What implant diameter and length are appropriate?
- Will the implant position support the final restoration?
Because implant success depends heavily on anatomical precision, CBCT enables more predictable planning, improved surgical safety, and better restorative outcomes.
Is a CBCT scan necessary before every dental implant procedure?
Not every implant case is equally complex, but modern implantology increasingly relies on CBCT because even straightforward cases benefit from accurate anatomical assessment.
A CBCT scan becomes particularly valuable when:
- Bone availability is uncertain
- The implant site is close to the mandibular nerve
- Implant placement is near the maxillary sinus
- Immediate implant placement is planned
- Guided surgery will be used
- Multiple implants are required
- Full-arch rehabilitation is being considered
- Previous bone loss or grafting has occurred
While some simple cases may appear manageable with conventional imaging, CBCT often reveals anatomical details that influence implant selection and positioning. This is one reason many implant specialists routinely incorporate CBCT into their planning workflow before surgery.
What information can a CBCT scan reveal that an OPG cannot?
An OPG provides a useful panoramic overview of the jaws and dentition, but it cannot accurately display anatomy in three dimensions.
CBCT can reveal details that panoramic imaging may not reliably show, including:
- True buccolingual bone width
- Ridge contour and morphology
- Cortical bone thickness
- Precise location of the mandibular canal
- Mental foramen position
- Maxillary sinus anatomy
- Nasal floor boundaries
- Bone defects and concavities
- Root relationships
- Three-dimensional implant angulation possibilities
This additional information allows clinicians to plan treatment with greater confidence and significantly reduces the uncertainty associated with implant surgery.
How does CBCT improve implant success rates?
CBCT does not directly guarantee implant success, but it improves the quality of treatment planning, which is one of the most important factors influencing long-term outcomes.
By providing detailed anatomical information before surgery, CBCT helps clinicians:
- Select the correct implant dimensions
- Avoid critical anatomical structures
- Improve implant angulation
- Identify bone deficiencies
- Determine the need for grafting procedures
- Enhance prosthetically driven planning
- Reduce surgical complications
Research has shown that CBCT-guided implant planning is associated with fewer nerve-related and sinus-related complications compared with traditional two-dimensional planning methods. When treatment decisions are based on accurate anatomical data, surgery becomes more predictable and restorative outcomes often improve.
How accurate are CBCT measurements for implant planning?
CBCT is highly accurate for evaluating implant sites and is widely used for measuring bone dimensions before surgery.
Clinicians can accurately assess:
- Vertical bone height
- Horizontal bone width
- Ridge morphology
- Implant envelope dimensions
- Distance to vital anatomical structures
Studies have demonstrated that CBCT measurements are significantly more accurate than panoramic radiography for implant planning. This level of precision is particularly important because implant treatment decisions often depend on differences measured in millimeters.
Accurate measurements help clinicians avoid placing implants that are too long, too wide, or positioned too close to anatomical structures such as nerves or the maxillary sinus.
What is guided implant surgery and why does it depend on CBCT?
Guided implant surgery is a digital workflow that allows implant placement to be planned virtually before surgery and then transferred accurately to the patient’s mouth using a surgical guide.
The process typically involves:
- Acquiring a CBCT scan
- Obtaining an intraoral digital scan
- Virtually positioning implants using planning software
- Designing a surgical guide
- Performing guided implant placement
CBCT serves as the anatomical foundation of this workflow because it provides the three-dimensional dataset needed to evaluate bone anatomy and determine implant positioning.
Without CBCT imaging, accurate guided surgery planning would not be possible because clinicians would lack the necessary spatial information required for digital treatment planning.
Can CBCT help identify whether bone grafting is required?
Yes. One of the most valuable benefits of CBCT is its ability to evaluate bone volume and morphology before surgery.
The scan helps clinicians determine:
- Whether adequate bone exists for implant placement
- If ridge augmentation is required
- Whether sinus lift procedures may be necessary
- The extent of existing bone loss
- The best surgical approach for the patient
Instead of discovering deficiencies during surgery, clinicians can identify these challenges beforehand and incorporate grafting procedures into the treatment plan if needed. This proactive approach often improves treatment predictability and reduces unexpected intraoperative complications.
How does CBCT help avoid nerve injury during implant placement?
Nerve injury is one of the most serious potential complications associated with implant surgery, particularly in the posterior mandible where implants may be placed close to the inferior alveolar nerve.
CBCT allows clinicians to visualize:
- The mandibular canal
- Inferior alveolar nerve pathway
- Mental foramen
- Accessory anatomical structures
Because these structures can be viewed in three dimensions, clinicians can accurately measure the available distance between the planned implant and the nerve. This information helps establish safe surgical margins and significantly reduces the risk of nerve-related complications such as numbness, altered sensation, or nerve trauma.
Is CBCT safe for patients considering dental implants?
Yes. CBCT is generally considered safe when prescribed appropriately and performed according to current imaging guidelines. Modern implant-planning protocols increasingly utilize:
- Low-dose acquisition settings
- Small field-of-view imaging
- Advanced image reconstruction technologies
- Optimized exposure protocols
In addition, clinicians follow the ALARA principle (As Low As Reasonably Achievable), meaning imaging is only performed when the expected diagnostic benefit justifies the radiation exposure.
For implant planning, the information gained from CBCT frequently outweighs the relatively small increase in exposure compared with conventional panoramic radiography because it directly contributes to safer and more predictable treatment planning.
How is artificial intelligence changing CBCT implant planning?
Artificial intelligence is becoming an increasingly valuable support tool in implant planning workflows. Modern AI-assisted systems can help automate tasks such as:
- Nerve tracing
- Anatomical landmark identification
- Sinus segmentation
- Implant site measurements
- Structured report drafting
- Workflow organization
These technologies improve efficiency and consistency while reducing repetitive manual processes.
At Nidaan, AI-assisted workflows help support CBCT reporting by organizing anatomical observations and assisting with report preparation. However, all findings continue to undergo radiologist review and validation before final reporting.
The goal of AI is not to replace clinical expertise. Its role is to improve efficiency, reduce variability, and support better decision-making.
When should an implantologist choose CBCT instead of relying only on OPG?
An implantologist should strongly consider CBCT whenever implant treatment depends on precise anatomical information that cannot be reliably assessed using two-dimensional imaging alone.
CBCT is particularly recommended when:
- Implant positioning must be highly precise
- Bone dimensions influence treatment decisions
- Guided surgery is planned
- Immediate implant placement is considered
- Sinus anatomy may affect surgery
- Multiple implants are being placed
- Full-arch rehabilitation is planned
- Significant bone loss exists
- Vital anatomical structures are nearby
A practical clinical rule is simple: If implant safety, implant positioning, restorative outcomes, or treatment predictability depend on accurate three-dimensional visualization, CBCT should be part of the planning process. Modern implant dentistry is increasingly digital and prosthetically driven. In that environment, CBCT is no longer simply an imaging option, it is often the foundation upon which predictable implant treatment is built.