TL;DR
- CBCT is a 3D dental imaging system, unlike traditional 2D X-rays
- It captures 150–600 images per scan, enabling full anatomical visualization
- Improves diagnostic accuracy in implants and endodontics (e.g., 91.8% vs 78.4% success rates)
- Uses moderate radiation (10–200 µSv) higher than X-rays but far lower than medical CT
- Essential for complex dental cases, not routine checkups
- Represents a shift from estimation → precision-driven dentistry
If traditional dental X-rays already work, why are dentists increasingly recommending CBCT scans?
Because modern dentistry is no longer limited by what is visible it is limited by what is measurable and predictable. And that’s where CBCT changes the equation.
What Is a CBCT Scan in Dentistry?
A CBCT (Cone Beam Computed Tomography) scan is a 3D dental imaging technology that captures detailed views of teeth, jawbone, nerves, and surrounding structures using a rotating cone-shaped X-ray beam.
In simple terms:
CBCT = 3D dental imaging
X-ray = 2D flat image
This difference is not just visual, it directly impacts diagnostic accuracy and treatment outcomes.
The Real Clinical Difference
Traditional dental X-rays compress complex anatomical structures into a flat image. This means:
- overlapping structures
- hidden pathologies
- no depth perception
CBCT, on the other hand, creates a volumetric dataset, allowing dentists to:
- view anatomy in multiple planes (axial, sagittal, coronal)
- isolate specific structures
- measure depth and spatial relationships accurately
Clinical literature consistently supports this: CBCT provides a multi-planar, volumetric view with significantly higher diagnostic precision than 2D imaging
Why This Matters in Practice
This shift is most relevant in cases where precision directly affects outcomes, such as:
- implant planning (bone density, nerve location)
- root canal diagnosis (hidden canals, fractures)
- orthodontics (jaw relationships, airway analysis)
- impacted teeth and surgical planning
In these scenarios, the limitation of 2D imaging is not just technical, it becomes a clinical constraint.
CBCT is not simply an upgraded X-ray. It is a transition from approximation to measurable accuracy and in dentistry, where millimeters determine success or failure, that distinction is critical.

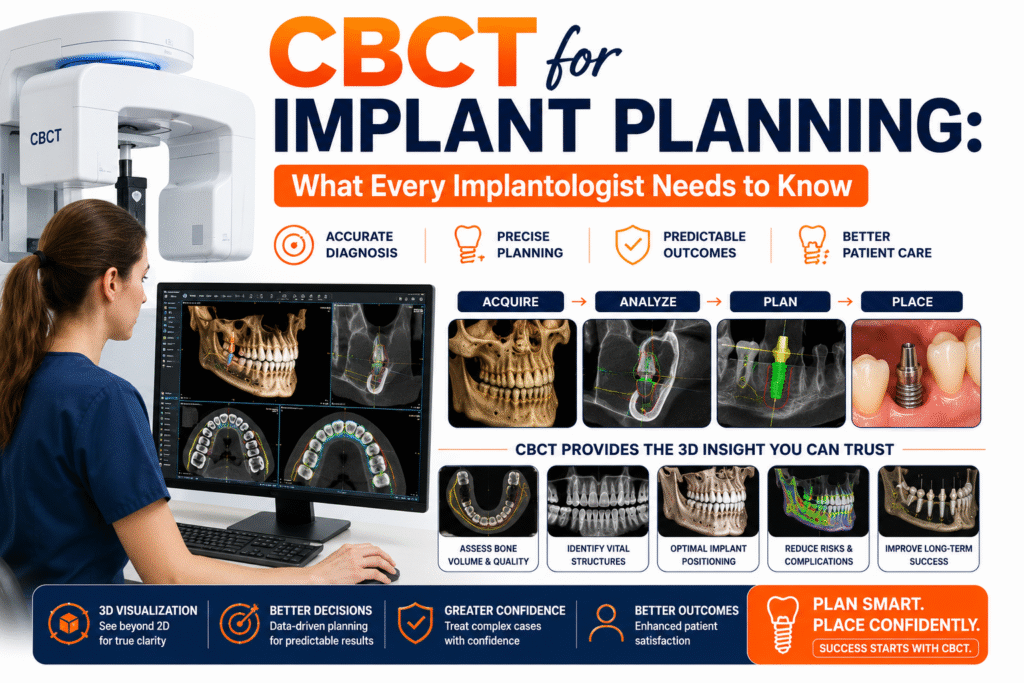
How CBCT Works: The Science Behind the Scan
A CBCT scan works by rotating a cone-shaped X-ray beam around the patient’s head in a single motion, capturing hundreds of images that are reconstructed into a detailed 3D model of dental structures.
What Actually Happens During a CBCT Scan
Instead of taking one or two flat images like traditional X-rays, CBCT follows a different process:
- The machine rotates once around the patient’s head
- During this rotation, it captures 150–600 individual images
- These images are then processed using specialized software
- The system reconstructs them into a 3D volumetric dataset
Each scan typically produces: 100–200 MB of imaging data.
This is significantly higher than conventional X-rays, which usually generate only a few megabytes.
Why This Matters Clinically
This large dataset is not just about size it represents depth, angles, and structure.
Dentists can:
- view cross-sections of teeth and bone
- analyze structures layer by layer
- rotate and zoom into specific regions
- measure distances with high precision
In practical terms: CBCT converts imaging from visual estimation → measurable anatomy
The Key Technical Advantage: Single-Rotation Imaging
One of the most important differences between CBCT and traditional CT imaging is: Single-rotation acquisition
- CBCT captures the entire region in one continuous rotation
- Medical CT scans capture multiple slices sequentially
This makes CBCT:
- faster
- more efficient
- more comfortable for patients
confirms that this single-rotation approach allows full-volume imaging with improved speed and patient comfort.
What Makes CBCT More Useful Than Just “More Data”
The real advantage is not the number of images, it’s the context those images provide.
Instead of seeing: a flattened projection
Dentists now see:
- full anatomical relationships
- bone thickness and density
- nerve pathways and proximity
- hidden structures that 2D imaging cannot reveal
CBCT doesn’t just capture better images. It captures complete anatomical context in a single scan and that shift from isolated images to full 3D understanding is what enables predictable, precision-based dentistry.
Conventional Dental X-Rays: What They Do Well
Conventional dental X-rays remain the first-line imaging tool for routine dental care because they are fast, accessible, and clinically effective for basic diagnosis despite their limitations in depth and detail.
Why Dentists Still Rely on X-Rays
Before we position CBCT as “advanced,” it’s important to understand something clearly: You and most patients still benefit from conventional X-rays in everyday dentistry.
They are not outdated, they are purpose-built for routine care.
Common types include:
- Bitewing X-rays
- Periapical X-rays
- Panoramic (OPG) X-rays
These are widely used because they are:
- quick to perform
- cost-effective
- low in radiation exposure
- available in almost every dental setup
For a dentist managing daily clinical flow, this matters.
Where X-Rays Perform Best (Clinical Reality)
In real-world practice, you’ll see that X-rays are highly effective for:
- detecting cavities
- evaluating bone levels
- monitoring periodontal conditions
- performing general dental checkups
For these use cases:
You don’t need 3D imaging
You need speed, clarity, and efficiency
And that’s exactly what X-rays provide.
The Core Limitation (And Why It Matters)
However, there’s one limitation that you cannot ignore: X-rays are 2D representations of 3D structures
This leads to:
- overlapping anatomical structures
- lack of depth perception
- difficulty identifying hidden lesions or fractures
In simple cases, dentists can work around this. But when complexity increases: This limitation becomes a clinical risk factor
Where You Start Seeing the Gap
Let’s say you are dealing with:
- a suspected root fracture
- implant planning near a nerve
- complex root canal anatomy
In these situations:
- X-rays may miss critical details
- Or worse, give a false sense of clarity
This is where decision-making shifts from: “Is this good enough?” to “Is this precise enough?” This limitation is well recognized in clinical imaging guidelines.
As noted by the American Academy of Oral and Maxillofacial Radiology:
“CBCT should be considered when conventional radiographic imaging does not provide adequate information for diagnosis or treatment planning.”
This reflects a practical reality in dentistry:
2D imaging works well for routine evaluation
But in complex cases, it may not provide sufficient diagnostic confidence
The Real Positioning (No Overclaim)
It’s important not to oversimplify this comparison.
CBCT is not a replacement for X-rays
And X-rays are not inferior they are context-specific
Think of it this way:
- X-rays = screening and routine evaluation
- CBCT = precision and complex planning
Conventional X-rays continue to play a critical role because they are:
- Efficient
- Practical
- Clinically sufficient for most routine cases
But the moment precision becomes non-negotiable: their limitations become visible
And that’s where dentistry begins to transition from routine imaging → precision imaging
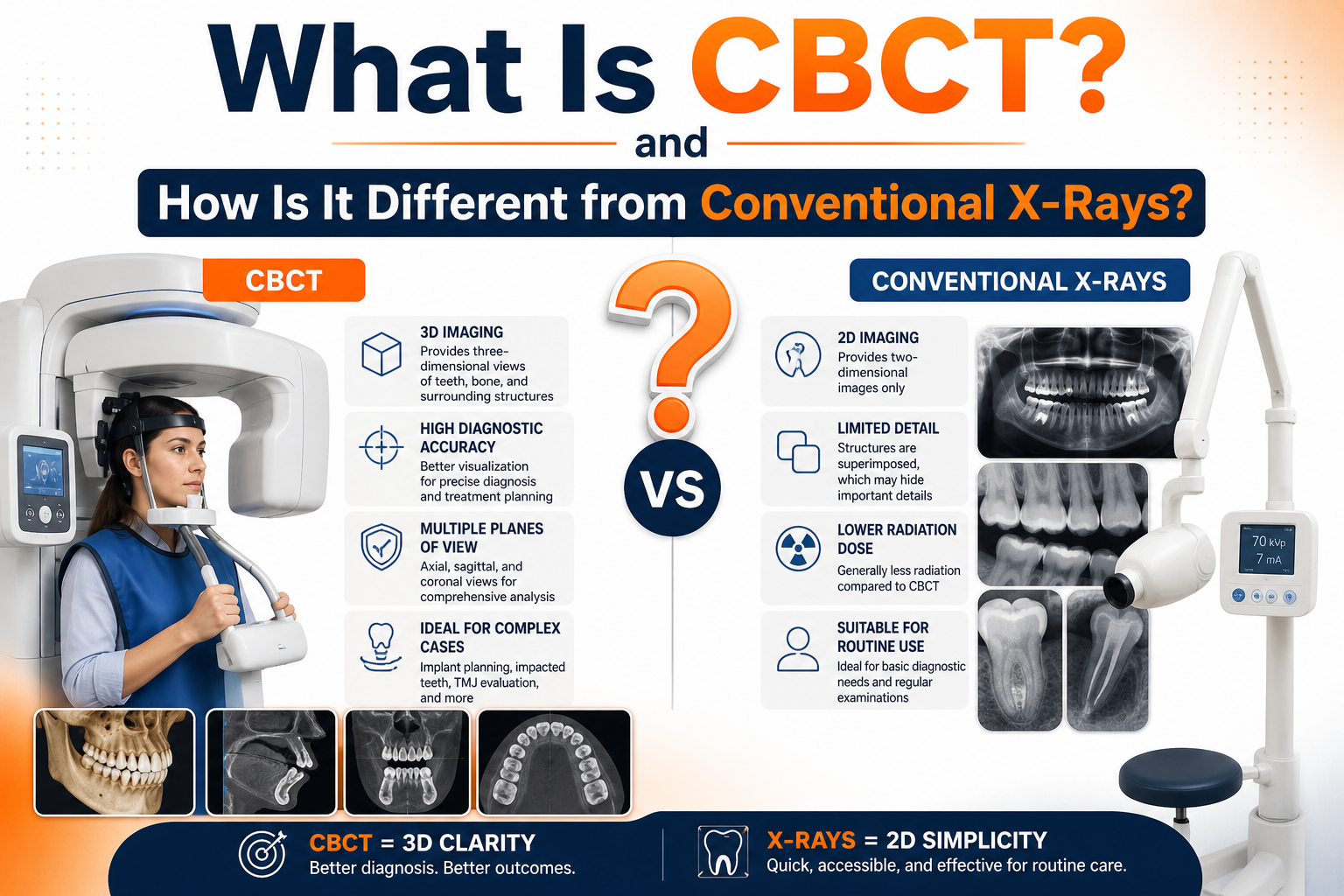
CBCT vs Conventional X-Rays: The Core Difference
The fundamental difference between CBCT and conventional X-rays lies in depth. CBCT provides a true 3D understanding of anatomy, while X-rays offer a flat 2D projection making them suitable for different clinical purposes.
The Real Question: What Are You Trying to See?
When you compare CBCT and X-rays, the question is not: “Which is better?”
It is: “What level of detail and certainty do you need?”
Because in clinical practice, imaging is not about visibility alone it’s about decision-making confidence.
The Core Difference Explained Simply
At the center of this comparison is one concept:
Depth vs Flatness
| Factor | CBCT Scan | Conventional X-Ray |
| Image Type | 3D volumetric | 2D flat |
| Detail Level | High | Moderate |
| Depth Visibility | Yes | No |
| Data Output | 100–200 MB | Few MB |
| Use Case | Complex diagnosis | Routine checks |
What This Means for You (Clinical Perspective)
With CBCT, dentists can:
- rotate and examine structures from multiple angles
- measure bone dimensions accurately
- identify spatial relationships between nerves, roots, and bone
With X-rays, they:
- see a compressed image
- infer depth based on experience
- rely on approximation in complex cases
This is a critical shift:
From interpretation based on projection
To analysis based on actual structure
Why This Difference Becomes Critical
In routine scenarios, you don’t need depth.
But when you are dealing with:
- implant placement near nerves
- hidden infections
- multi-root canal anatomy
- impacted teeth
Flat imaging introduces uncertainty.
And in dentistry: Small uncertainties can lead to major clinical consequences
Evidence-Based Insight
Clinical studies consistently show that CBCT provides:
- higher diagnostic accuracy
- better sensitivity and specificity
- improved detection of complex anatomy
This is because CBCT captures: true spatial relationships, not approximations
The Practical Takeaway
You should not think of CBCT and X-rays as competitors.
They operate at different levels:
- X-rays → screening and basic evaluation
- CBCT → precision diagnosis and planning
When the case is simple: X-rays are efficient and sufficient
When the case is complex: CBCT becomes necessary for clarity
The difference between CBCT and X-rays is not just technological.
It represents a shift in dentistry: From seeing surfaces to understanding structures in full context and that shift is what enables predictable, precision-driven treatment outcomes.
Why CBCT Is More Accurate in Diagnosis
CBCT improves diagnostic accuracy by eliminating anatomical overlap and providing true 3D visualization allowing dentists to detect conditions that are often missed or misinterpreted in 2D X-rays.
The Real Problem with Traditional Imaging
When you rely on conventional X-rays, you’re often working with:
- overlapping structures
- limited angles
- no depth perception
This means: You are interpreting a compressed version of reality
In many routine cases, this works.
But in complex scenarios: It introduces uncertainty into diagnosis and treatment planning
How CBCT Removes That Uncertainty
CBCT changes this by giving you access to actual anatomical structure, not projections.
With CBCT, dentists can:
- isolate individual teeth and roots
- view cross-sections layer by layer
- detect lesions hidden behind overlapping structures
- measure bone and spacing with precision
Instead of guessing what lies behind an image: You are seeing it directly
Where This Makes the Biggest Difference
You’ll notice the impact of CBCT most in cases where precision matters:
- Implant Planning
- exact bone height and width
- nerve location
- implant angulation
- Endodontics (Root Canals)
- hidden or accessory canals
- periapical infections
- root fractures
- Oral Pathology
- cysts and lesions
- early-stage infections
- structural abnormalities
In these cases: Missing small details can lead to failed or delayed treatment
What the Data Shows
Clinical data reinforces this difference:
- Implant planning success: 91.8% with CBCT vs 78.4% with panoramic X-rays
- Endodontic diagnostic accuracy: ~73.6% accuracy with CBCT, significantly higher than 2D imaging
- Studies consistently report higher sensitivity and specificity with CBCT in complex cases
Why Accuracy Matters More Than You Think
In dentistry, errors are rarely dramatic; they are subtle.
A missed canal
A slight misalignment
An undetected fracture
These small gaps can lead to:
- treatment failure
- repeat procedures
- complications
CBCT reduces this risk by: improving visibility → accuracy → predictability
The Shift in Clinical Decision-Making
With X-rays, dentists often rely on: experience + interpretation
With CBCT, they rely on: data + measurable anatomy
This doesn’t replace clinical expertise, it enhances it. CBCT is more accurate not because it is “better technology,” but because it: removes ambiguity from diagnosis
And in clinical practice: Less ambiguity = better outcomes
That’s why CBCT is increasingly used when treatment decisions require confidence, not estimation.
Radiation: Is CBCT Safe Compared to X-Rays?
CBCT uses more radiation than standard dental X-rays, but significantly less than medical CT scans making it a controlled, mid-dose imaging option used only when clinically necessary.
The Concern You Naturally Have
If your dentist recommends CBCT, the first question that comes to mind is: “Is this safe?”
And that’s a valid concern. Because unlike routine X-rays, CBCT involves higher exposure levels but the context matters.
Understanding the Actual Radiation Levels (With Clinical Benchmarks)
Let’s break it down with real clinical data:
CBCT Radiation Range
- Typical CBCT dose: 10–200 µSv (microsieverts)
- Most commonly used range in practice: 50–150 µSv per scan
Comparison With Other Dental Imaging
- Intraoral X-ray: ~1–8 µSv
- Panoramic (OPG): ~4–30 µSv
- CBCT vs panoramic: Can be 2–25× higher depending on field of view (FOV)
Comparison With Medical CT
- CBCT (average): ~1.8 mSv
- Medical CT scan: often >2.5 mSv or significantly higher
That’s roughly 30% lower radiation than medical CT for localized imaging
Real-World Comparisons (For Context)
- CBCT ≈ 3–20 days of natural background radiation
- Dental X-ray ≈ 1 day of background radiation
- Chest X-ray ≈ 10 days of background radiation
- Abdominal CT ≈ years of background exposure
In many cases, a CBCT scan is comparable to a short period of everyday environmental exposure
What This Means Clinically (Important for Dentists)
Radiation is not evaluated in isolation, it’s evaluated in risk vs diagnostic benefit.
Key clinical insights:
- CBCT provides higher diagnostic yield per exposure unit
- Dose varies significantly based on:
- field of view (FOV)
- machine settings
- scan region
Recent studies emphasize: Proper protocol selection can optimize dose without compromising image quality
Also: Dental imaging contributes <1% of total medical radiation exposure annually
The ALARA Principle (Non-Negotiable Standard)
Dentists follow: ALARA As Low As Reasonably Achievable
Which means:
- CBCT is used only when necessary
- exposure is minimized
- scan area is restricted
Modern protocols also focus on: FOV-based dose reduction + optimized parameters
The Real Risk vs Benefit Equation
Here’s the actual clinical reality:
- Low-detail imaging → risk of missed diagnosis
- High-precision imaging → slightly higher exposure but better outcomes
In complex cases: Not using CBCT can increase:
- diagnostic errors
- surgical risks
- treatment failure
What This Means for You (Practical Perspective)
Radiation is not just about numbers, it’s about justification. Dentists don’t recommend CBCT for routine cases.
They recommend it when:
- 2D imaging is insufficient
- precision is critical
- treatment decisions depend on accuracy
So the question shifts from: “Is there radiation?” to “Is this level of imaging necessary for this case?”
The ALARA Principle (Clinical Standard)
Dentists follow a strict safety guideline: ALARA which means As Low As Reasonably Achievable
This means:
- CBCT is used only when needed
- exposure settings are optimized
- field of view is limited to the area of interest
confirms that modern guidelines emphasize justification and dose optimization, ensuring responsible use.
How Technology Improves Safety
Modern CBCT systems are designed to:
- adjust radiation based on the scan area (FOV)
- reduce unnecessary exposure
- deliver high-quality images with optimized dose
This ensures: You get maximum diagnostic value with controlled exposure
The Real Risk vs Benefit Equation
Here’s the clinical reality:
- Low-detail imaging → risk of missed diagnosis
- High-precision imaging → slightly higher exposure but better outcomes
In complex cases: Not using CBCT can sometimes carry more risk than using it
Because:
- undetected issues lead to complications
- inaccurate planning leads to failures
CBCT is not a routine imaging tool and it’s not meant to be. It is a precision tool used selectively.
When used appropriately: The benefit of accurate diagnosis far outweighs the controlled radiation risk and that’s why dentists rely on it when certainty matters more than approximation.
When Dentists Recommend CBCT Scans
CBCT scans are recommended when clinical decisions require precision that 2D X-rays cannot provide particularly in cases involving implants, complex anatomy, or uncertain diagnosis.
The Key Principle: Not Routine, But Purpose-Driven
CBCT is not used for every patient and that’s intentional.
You won’t need CBCT for routine checkups
But you may need it when accuracy directly impacts outcomes
Dentists follow a simple rule: Use CBCT only when 2D imaging is insufficient
When You’ll Most Likely Need a CBCT Scan
Let’s break it down by real clinical scenarios you or your dentist may encounter:
1. Dental Implants (Most Common Use Case)
If you’re planning an implant, CBCT becomes critical.
Dentists use it to:
- measure bone height, width, and density
- identify nerve pathways
- plan implant angulation precisely
Without CBCT: Implant placement relies on estimation
With CBCT: It becomes data-driven and predictable
2. Root Canal Treatment (Endodontics)
In complex cases, standard X-rays may not reveal:
- hidden or extra canals
- root fractures
- persistent infections
CBCT helps dentists:
- visualize root morphology in 3D
- detect issues missed in 2D imaging
For you, this means: fewer failed treatments and retreatments
3. Impacted Teeth & Surgical Cases
For impacted wisdom teeth or surgical extractions:
- exact tooth position matters
- nerve proximity is critical
CBCT provides: precise location and orientation
This reduces the risk of:
- nerve injury
- surgical complications
4. Orthodontics & Jaw Assessment
In orthodontic planning, CBCT helps evaluate:
- jaw alignment
- facial structure
- airway space
Compared to 2D cephalometric analysis: 3D imaging provides more accurate structural relationships
5. TMJ (Jaw Joint) Disorders
If you have jaw pain, clicking, or limited movement:
CBCT can assess:
- joint structure
- bone changes
- degenerative conditions
This enables: more targeted diagnosis and treatment planning
6. Sinus, Cysts, and Pathology Detection
CBCT is also used when dentists suspect:
- cysts or tumors
- sinus involvement
- infections extending beyond teeth
Because: 2D X-rays may miss boundaries and depth
CBCT defines: the exact extent of the condition
What This Means for You
If your dentist recommends CBCT, it usually means: Your case requires clarity, not approximation
It is not about “extra testing”
It is about: reducing uncertainty before treatment begins
Clinical Insight
Modern guidelines consistently emphasize: CBCT should be used only when it adds diagnostic value beyond 2D imaging
This ensures:
- responsible use
- patient safety
- clinically justified decisions
CBCT is not about doing more imaging. It’s about doing the right imaging at the right time. When complexity increases, so does the need for precision.
And in those moments: CBCT becomes the difference between informed treatment → predictable outcomes.
Speed, Comfort, and Patient Experience
CBCT scans are designed to be fast, non-invasive, and comfortable capturing complete 3D imaging in a single rotation within seconds, with minimal effort required from you.
What You Actually Experience During a CBCT Scan
If you’ve never had a CBCT scan before, here’s what you can expect:
- You either stand or sit in position
- Your head is stabilized gently
- The machine rotates around you once
- The scan completes in a few seconds
There is:
no pain
no injections
no preparation required
From your perspective, it feels similar to a panoramic X-ray but faster and more efficient.
Why CBCT Is Faster Than You Expect
Unlike traditional medical CT scans that capture images slice by slice, CBCT works differently: It captures the entire region in one continuous rotation
This means:
- no repeated positioning
- no multiple exposures
- no long scanning time
confirms that CBCT’s single-rotation acquisition makes it significantly faster and more patient-friendly.
How This Improves Your Comfort
Speed directly affects comfort.
Because the scan is quick:
- you don’t need to stay still for long
- there is less chance of movement errors
- the process feels less intimidating
For you, especially if you’re anxious about dental procedures: shorter scan time = better overall experience
Why Dentists Prefer This Workflow
From a clinical perspective, faster imaging also means:
- quicker diagnosis
- reduced chair time
- smoother workflow in busy practices
Instead of waiting for multiple images or retakes: dentists get a complete dataset almost instantly
This allows them to:
- review results immediately
- plan treatment faster
- communicate findings clearly
Where This Matters Most
You’ll notice the benefit of CBCT speed and comfort in:
- complex cases requiring immediate decisions
- patients who struggle to stay still
- situations where multiple X-rays would otherwise be needed
Instead of taking several images: one CBCT scan provides everything in a single step
CBCT is not just about better imaging, it’s about better experience for you and better efficiency for your dentist.
Faster scan
Less discomfort
More complete information
And that combination makes it especially valuable when precision and time both matter.
Cost and Accessibility: Is CBCT Expensive?
CBCT scans are more expensive than standard dental X-rays because they involve advanced 3D imaging, higher data processing, and specialized interpretation but they remain more affordable than medical CT scans and are becoming increasingly accessible in modern dentistry.
Why CBCT Costs More Than X-Rays
If you compare CBCT with traditional X-rays, the cost difference is expected.
Because you’re not getting a single flat image you’re getting:
- 3D volumetric imaging
- 150–600 captured images per scan
- high-resolution datasets (100–200 MB)
- advanced software reconstruction
- detailed clinical analysis
So practically: You are paying for depth, precision, and decision-making clarity
Why It’s Still More Affordable Than Medical CT
Despite being advanced, CBCT is designed specifically for dental use.
That makes it:
- lower cost than hospital CT scans
- faster and more efficient
- focused on localized imaging (not full-body scanning)
confirms that CBCT systems are more cost-efficient than conventional CT, which is why they are widely adopted in dental practices.
Accessibility Is Increasing Rapidly
Earlier, CBCT was limited to hospitals or high-end setups.
Today, you’ll see it in:
- dental imaging centers
- specialized diagnostic facilities
- advanced dental clinics
Market data reflects this shift: The global CBCT market is projected to reach $1.77 billion by 2034, growing steadily due to implantology and advanced diagnostics
This tells you one thing: CBCT is moving from specialized → standard in complex dental care
The Real Question: Cost or Consequence?
When you evaluate CBCT, the better question is not: “Is it expensive?”
But: “What is the cost of not having accurate imaging?”
Because in complex cases:
- misdiagnosis leads to failed treatments
- incorrect planning leads to complications
- repeat procedures increase overall cost
In that context: CBCT often reduces long-term clinical and financial risk
When the Cost Is Justified
You’ll find CBCT most justified when:
- implant placement requires precision
- anatomy is complex or unclear
- previous treatment has failed
- surgical planning is involved
In these cases: Accuracy is not optional, it’s critical.
CBCT is more expensive than routine X-rays but that’s because it serves a different purpose.
X-rays = efficiency
CBCT = precision
And when precision directly impacts outcomes: The value of CBCT outweighs its cost. It’s not about paying more, it’s about reducing uncertainty where it matters most.
The Future of Dental Imaging: AI + CBCT
The future of dental imaging lies in combining CBCT with AI-driven analysis where high-quality 3D data is enhanced by intelligent tools to support faster, more consistent, and clinically relevant decision-making.
The Shift: From Imaging to Intelligence
CBCT already gives dentists complete 3D visibility. But the next evolution is not just about seeing more, it’s about understanding faster and more consistently.
This is where AI comes in. Instead of replacing clinical expertise, AI works as: a decision-support layer on top of CBCT imaging.
What AI Actually Does in CBCT Workflows
Modern AI systems can:
- highlight potential areas of concern (caries, bone loss, lesions)
- assist in measurements (bone density, spacing, angulation)
- support implant planning workflows
- improve consistency across cases
This means: You move from manual interpretation → assisted analysis
But importantly:
AI does not replace radiologists or dentists
It supports their clinical judgment
How Nidaan Integrates AI into Dental Imaging Workflows
At Nidaan Dental, AI is used as a structured support layer designed to assist radiologists and dentists in faster, more consistent interpretation, without replacing clinical judgment.
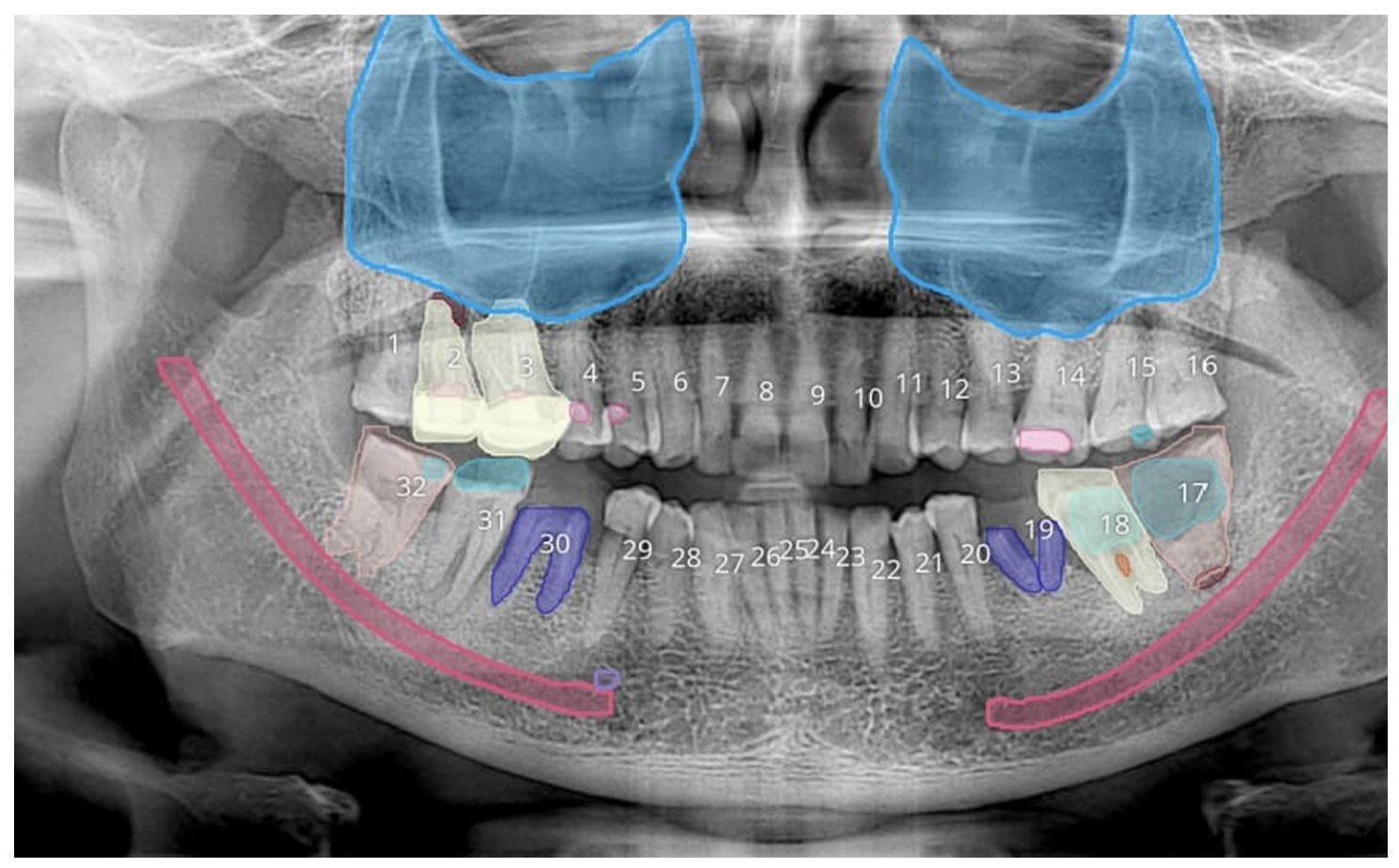
How Nidaan Uses AI in OPG (2D X-Ray) Reporting
In OPG imaging, AI is applied at the screening and visualization level.
Here’s how it works in practice:
- AI processes the X-ray image immediately after capture
- It marks potential abnormalities such as:
- caries
- bone loss
- impacted teeth
- radiolucent or radiopaque areas
- These findings are presented using color-coded overlays
This allows:
You (as a dentist) to quickly identify areas that need attention
Faster initial case understanding before detailed review
But importantly: These markings are indicative, not diagnostic
They act as a visual aid, helping you focus not replacing your evaluation.
How Nidaan Uses AI in CBCT Reporting
In CBCT workflows, AI plays a different role.
Instead of marking only, it supports report creation and structuring.
- AI assists in drafting CBCT reports
- It organizes imaging findings into a structured format
- It helps highlight:
- anatomical landmarks
- potential areas of concern
- measurement references
This enables:
Faster report generation
Reduced manual effort
Lower chances of missing key observations
However: The final report is always reviewed, validated, and concluded by a radiologist
The Role of Radiologists (Critical Layer)
Nidaan’s workflow is intentionally designed to maintain clinical accountability.
- AI provides:
- speed
- structure
- preliminary insights
- Radiologists provide:
- interpretation
- validation
- final diagnosis
This ensures:
No over-reliance on automation
No compromise on diagnostic accuracy
Why This Matters for You (Dentist Perspective)
In daily practice, time and clarity are critical.
With this integration, you get:
- faster initial screening (via AI-marked OPGs)
- structured CBCT reports for easier review
- an additional validation layer in complex cases
Instead of spending time identifying obvious patterns: You can focus on clinical decisions and treatment planning.
The Right Way to Understand AI in Dentistry
There is a common misconception that AI will replace doctors.
In real workflows, the model is much more practical:
- CBCT / OPG → provides raw imaging data
- AI → highlights, structures, and assists
- Radiologist / Dentist → interprets and decides
At Nidaan, AI is not positioned as a replacement, it is positioned as an efficiency and accuracy layer.
Technology enhances speed and consistency
Expertise ensures correctness and clinical reliability
And that combination defines the future of dental imaging: Data-supported, radiologist-led, precision-driven care

CBCT vs X-Ray, Which One Is Better?
CBCT is not “better” than X-rays in all situations; it is more suitable for complex cases, while conventional X-rays remain the preferred choice for routine dental evaluation.
The Common Misunderstanding
When you first hear about CBCT, it’s natural to think: “If it’s more advanced, shouldn’t it replace X-rays?”
But in clinical practice, that’s not how decisions are made.
Dentists don’t choose imaging based on “better technology”
They choose based on: what the case actually requires
The Right Way to Compare Them
Instead of asking: “Which is better?”
You should ask: “Which is appropriate for this situation?”
Because CBCT and X-rays serve different clinical roles.
When X-Rays Are the Right Choice
You’ll see conventional X-rays used when:
- routine dental checkups are needed
- cavities or basic bone levels are being assessed
- quick, low-cost imaging is sufficient
In these scenarios: X-rays are efficient, accessible, and clinically adequate
When CBCT Becomes Necessary
CBCT is recommended when:
- precision is critical
- anatomy is complex
- treatment planning involves risk (implants, surgery)
For example:
- implant placement near nerves
- root canal cases with hidden anatomy
- impacted teeth with unclear positioning
Here:
2D imaging is not enough
Depth and spatial understanding become essential
What Clinical Evidence Suggests
Clinical consensus consistently supports this distinction:
Conventional X-rays remain suitable for routine imaging
CBCT is increasingly the standard for complex diagnosis
This is not about replacement, it’s about appropriate application.
What This Means for You
If your dentist chooses:
- X-rays → your case is likely straightforward
- CBCT → your case requires higher precision
So the recommendation itself tells you something important: The level of imaging reflects the complexity of your condition
The Practical Framework
You can think of it simply:
- X-rays → screening and routine care
- CBCT → precision and advanced planning
Both are essential. They just operate at different levels of detail.
CBCT vs X-ray is not a competition. It’s a clinical decision based on need. The goal is not to use the most advanced tool. It’s to use the right tool for the right level of certainty
And in modern dentistry: That balance between efficiency and precision defines better outcomes.
Experience premium before its late
If your dentist recommends a CBCT scan, it’s usually because your case requires a level of precision that standard X-rays cannot provide. The goal is not more imaging, it’s better decision-making before treatment begins.
For dentists and clinics looking for high-precision imaging, structured radiology reporting, and advanced diagnostic support:
You can visit our CBCT & OPG Centre or contact us directly.
Because unlike multi-specialty labs, Nidaan is a B2B partner dedicated exclusively to dentistry. With a 40-year legacy, 1200+ dentist partners, and cutting-edge CBCT and AI solutions, we empower practices with faster, safer, and more precise diagnostics.
Whether you’re a patient trying to understand your scan or a dentist aiming for precision: The right imaging partner makes a measurable difference.
Because in modern dentistry: Accuracy at the diagnostic stage defines the outcome of the treatment.
FAQs
1. What is a CBCT scan in dentistry?
A CBCT (Cone Beam Computed Tomography) scan is a 3D dental imaging technique that captures detailed views of your teeth, jawbone, nerves, and surrounding structures in a single scan.
Unlike traditional X-rays that show flat images, CBCT allows dentists to analyze depth, angles, and spatial relationships, which is essential for accurate diagnosis and treatment planning in complex cases.
2. Is CBCT better than traditional dental X-rays?
CBCT is not universally “better” ; it is more suitable for specific situations.
- For routine checkups, cavities, and basic assessments → X-rays are sufficient
- For implants, complex root canals, or unclear anatomy → CBCT provides higher precision
In simple terms:
X-rays = routine screening
CBCT = advanced diagnostic clarity
3. Is CBCT safe for patients?
Yes, CBCT is considered safe when used appropriately. It uses controlled radiation levels (typically 10–200 µSv), which are higher than standard dental X-rays but significantly lower than medical CT scans.
Dentists follow strict safety protocols like the ALARA principle (As Low As Reasonably Achievable), ensuring CBCT is only recommended when the diagnostic benefit outweighs the exposure.
4. Why do dentists use CBCT for dental implants?
CBCT is essential for implant planning because it provides a complete 3D view of bone structure and nerve location.
With CBCT, dentists can:
- measure bone density and thickness
- identify exact nerve pathways
- determine ideal implant position and angulation
This reduces risks such as nerve damage or implant failure and leads to more predictable long-term outcomes.
5. Does a CBCT scan hurt?
No, a CBCT scan is completely painless and non-invasive.
You simply stand or sit still while the machine rotates around your head. There are no injections, no discomfort, and no recovery time required.
6. How long does a CBCT scan take?
The actual scan usually takes just a few seconds, as the machine completes imaging in a single rotation.
Including positioning and setup, the entire process is quick and efficient, making it comfortable even for patients who are anxious or have difficulty sitting still for long periods.
7. Is CBCT more expensive than X-rays?
Yes, CBCT scans are more expensive than standard dental X-rays because they involve:
- advanced 3D imaging technology
- larger data processing
- detailed clinical analysis
However, in complex cases, CBCT can prevent diagnostic errors and repeat procedures, which may reduce overall treatment costs in the long run.
8. Can CBCT detect infections or hidden dental problems?
Yes, CBCT is significantly more effective at detecting conditions that may not be visible on 2D X-rays, such as:
- hidden infections
- cysts and lesions
- root fractures
- complex root canal anatomy
Because it shows structures in 3D, it allows dentists to identify issues earlier and more accurately.
9. Is CBCT necessary for root canal treatment?
In routine root canal cases, standard X-rays are often sufficient.
However, CBCT becomes important when:
- canals are complex or difficult to locate
- previous treatment has failed
- fractures or hidden infections are suspected
In such cases, CBCT helps dentists avoid missed canals and improve treatment success rates.
10. What is the radiation dose of a CBCT scan?
CBCT typically delivers 10–200 µSv of radiation, depending on the scan type and area being examined.
To put this into perspective:
It is higher than a standard dental X-ray
But significantly lower than a medical CT scan
Dentists carefully select CBCT only when necessary, ensuring the diagnostic benefit justifies the exposure.